

Translate this page into:
Upper arm brachial-axillary translocated superficial femoral vein for hemodialysis
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications and was migrated to Scientific Scholar after the change of Publisher.
A 55-year-old man with end-stage renal disease secondary to diabetes was referred to our department for permanent hemodialysis access. He had previously undergone three arteriovenous accesses (left radiocephalic arteriovenous fistulas [AVF]), left brachiocephalic AVF, and right brachiobasilic AVF). All of the accesses had failed in the first 6 months.
Preoperative evaluation showed diminutive basilic veins bilaterally, no evidence of central vein thrombosis in the upper extremities, no evidence of deep vein thrombosis in the lower extremities, and no suitable saphenous veins bilaterally. The patient underwent a right brachial artery-axillary vein autogenous access using reversed superficial femoral vein. The arterial anastomosis was performed to the brachial artery proximal to the antecubital crease, and the venous anastomosis was performed to the axillary vein within the axilla [Figure 1]. The superficial femoral vein was harvested through an incision that ran diagonally over the anteromedial aspect of the thigh [Figure 2]. The access matured in 4 weeks and has been used successfully for hemodialysis. The length of the vein available for cannulation was 13 cm. The patient has dialyzed through the access for the past 8 months without problems.
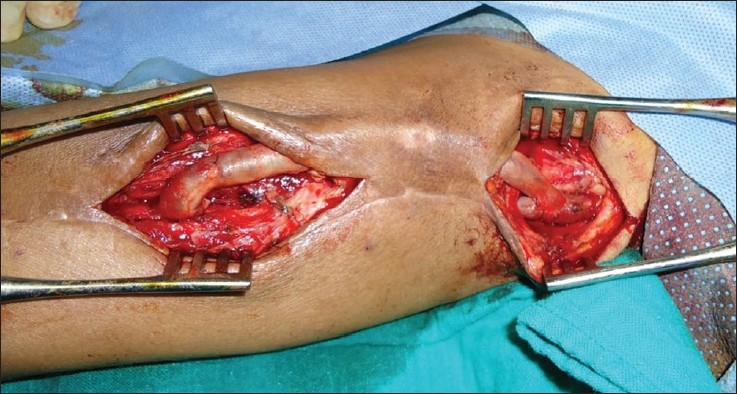
- Intraoperative view of right brachial artery-axillary vein translocated superficial femoral vein
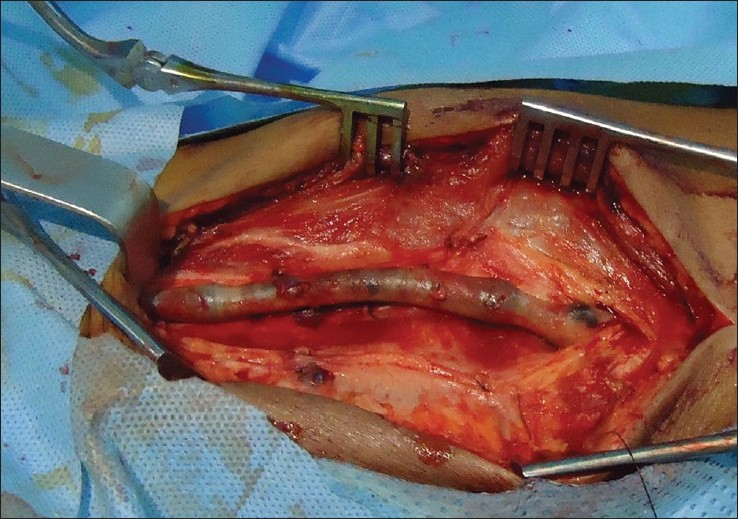
- Harvesting of superficial femoral vein
AVF are crucial in patients requiring long-term hemodialysis. The dialysis outcomes quality Initiatives guidelines emphasize placement of AVF for patients on hemodialysis.[1] This recommendation is based on studies that demonstrate enhanced patency for AVF compared with grafts. This preference for a native AVF has led many to perform some innovative access operations. Transposition of the brachial vein reported by Bazan and Shanzer[2] is characterized by a high incidence of complications and a long period to achieve maturation. Despite close monitoring and a high rate of secondary interventions, the patency rate was low.[3] Reported series of lower-extremity AV access have documented relatively poor patency rates and a high incidence of infection.[4] The use of autogenous saphenous vein for AVF in the thigh has met with limited success. Patency rates of 40% at 3 years, and fragility (two fatal bleeding complications) have been reported.[56]
Because of our satisfactory experience with the superficial femoral vein (SFV) for other arterial and venous reconstructions, we used this material for constructing arteriovenous access in the patient described. The diameter of SFV ranges from 6 to 10mm in adults.[7] The wall is thick, relative to the basilic and cephalic veins and may attenuate the requisite time necessary for maturation. The use of autogenous material should essentially eliminate the risk of graft infection.[8]
We did not use the SFV in the thigh because of the risk of occurrence of infection and distal limb ischemia secondary to steal syndrome especially since our patient was diabetic with long-standing end-stage renal disease and therefore at high risk of asymptomatic peripheral arterial obstructive disease.
Huber et al. reported on the outcome of 30 SFV translocations.[9] The primary, primary assisted, and secondary patency rates for the SFV were 79%, 91%, and 100%, respectively, at 12 months; and 67%, 86%, and 100%, respectively, at 18 months.
This technique appears to be a reasonable alternative for establishing durable AV access in patients requiring hemodialysis who had multiple previous failed upper-extremity access. Additional clinical experience with the procedure and longer follow-up will be necessary to assess its ultimate role as a standard alternative when upper-extremity AV access is problematic.
Source of Support: Nil
Conflict of Interest: None declared.
References
- National Kidney Foundation-K/DOQI clinical practice guidelines for vascular access: Update 2000. Am J Kidney Dis. 2001;37:S137-81.
- [Google Scholar]
- Transposition of the brachial vein: A new source for autologous arteriovenous fistulas. In: J Vasc Surg. Vol 40. 2004. p. :184-6.
- [Google Scholar]
- Autogenous brachial-brachial fistula for vein access.Haemodynamic factors predicting outcome and 1 year clinical data. Eur J Vasc Endovasc Surg. 2009;38:770-6.
- [Google Scholar]
- Results and complications of arteriovenous access dialysis grafts in the lower extremity: A five year review. Am Surg. 1996;62:188-91.
- [Google Scholar]
- Long-term results of saphenous vein graft arteriovenous fistulas. Am J Surg. 1980;140:387-90.
- [Google Scholar]
- Clinical experience with the saphena loop arteriovenous fistula on the thigh. Int Urol Nephrol. 1981;13:287-90.
- [Google Scholar]
- Use of superficial femoral vein for hemodialysis arteriovenous access. J Vasc Surg. 2000;31:1038-41.
- [Google Scholar]
- The superficial femoral-popliteal vein transposition fistula: Description of a new vascular access procedure. J Am Coll Surg. 2000;191:581-4.
- [Google Scholar]
- Patency of autogenous and polytetrafluoroethylene upper extremity arteriovenous hemodialysis accesses: A systematic review. J Vasc Surg. 2003;38:1005-11.
- [Google Scholar]




