

Translate this page into:
A case of paraneoplastic syndrome associated rapidly progressing glomerulonephritis in a patient with colon cancer
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Rapidly progressive crescenteric glomerulonephritis (RPGN) is often a consequence of systemic disease. We present a case of RPGN found in the setting of colo-rectal carcinoma, leaving paraneoplastic syndrome associated RPGN as the most likely etiology.
A 46-year-old African American female was admitted with a history of colon carcinoma managed with chemotherapy and partial colectomy. She had a normal creatinine 8 months prior to admission. Her creatinine was 3.1 mg/dl on the day of admission and her antinuclear antibodies, ANCA, antiglomerular basement membrane, antiproteinase-3 antibodies, and myeloperoxidase antibodies were negative. On the 3rd day of admission her creatinine was 4.5 mg/dl and urinalysis revealed active urine sediments. She underwent a renal biopsy, which revealed crescent-shaped mass of proliferating cells and leukocytes internal to bowman capsule along with thickening of periphery capillary walls, collapsed glomerular tufts and expanded mesangial areas with formation of mesangial nodules that stained periodic acid Schiff and silver positive on light microscopy. Electron microscopy showed thickening and segmental hyalinization of small size arteries and fibrosis in the interstitium. Immunofluorescence was negative for immune complexes [Figure 1]. She was managed with intravenous steroids and cyclophosphamide, and was discharged with a creatinine of 2.4 mg/dl.
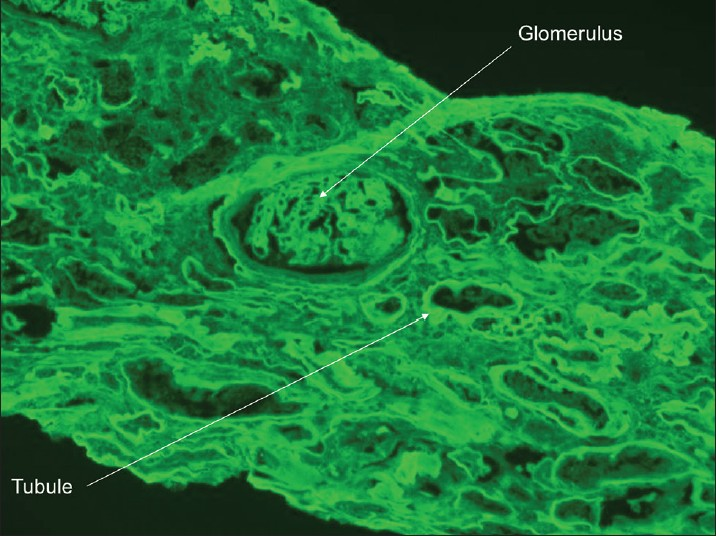
- Immunofluorescence IgG 10X: Linear staining along glomerular peripheral capillary walls and tubular basement membranes (2+). No specific vascular staining
The outcomes of malignancies are not limited only to tumor bulk or metastases. Malignancies can produce hormones, cytokines, or immunologic responses that have diffuse system impacts.[1] The development of unusual pathologies in cancer patients with no alternative etiology should raise suspicion towards a paraneoplastic syndrome. The glomerular damage in our patient is likely related to cytokine-mediated effects of malignancy, as evidenced by the lack of immune complexes on immunofluorescence.[2] Under the influence of various cytokines, a pro inflammatory state is maintained.[3] Such an environment could be analogous to the labile cellular milieu encountered in systemic vasculitis. It is not surprising, then, that the end organ consequences of both pathologies be similar as indicated by the RPGN observed in our patient.
References
- Cytokine patterns in patients with cancer: A systematic review. Lancet Oncol. 2013;14:e218-28.
- [Google Scholar]
- , Membranous nephropathy and cancer: Epidemiologic evidence and determinants of high-risk cancer association. Kidney Int. 2006;70:1510-7.
- [Google Scholar]
- Endothelium-neutrophil interactions in ANCA-associated diseases. J Am Soc Nephrol. 2012;23:1449-61.
- [Google Scholar]




