

Translate this page into:
Ceftazidime-induced myoclonus and encephalopathy in hemodialysis patient
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
A 49-year-old diabetic male on maintenance hemodialysis for 8 months presented with complaints of pain and swelling in the left ear. Investigation revealed hemoglobin of 7.4 g/dl; leukocyte count of 28,400 cells/μL; differential count polymorphs, 86% and lymphocytes, 9%. He was treated with ear packs and oral ciprofloxacin. However, the pain and swelling worsened. Computerized tomography scan of skull showed extensive damage of middle ear and ear ossicles [Figure 1] with skull bone erosions [Figure 2] suggestive of malignant otitis externa. Ceftazidime 1 g twice daily intravenously was added. Considering the potential life- threatening nature of illness, we gave a higher than his renal adjusted dose for ceftazidime. After 2 days of starting ceftazidime, the patient developed myoclonic movements of upper limb and was confused. Since patient was on ciprofloxacin for more than 2 weeks, it was stopped considering it might be contributing to the patient's condition. Magnetic resonance imaging of brain was normal and there was no evidence of extension of infection to brain. He developed generalized myoclonic movements with alteration in sensorium by 4th day of staring ceftazidime, requiring intensive care support. His myoclonus and encephalopathy was not showing any change in post dialysis period and was present during sleep also. Since his condition was worsening and no other identifiable causative factors were evident in clinical examination, ceftazidime was stopped. Two days later, his movements were reduced and sensorium improved. By 5th day the patient was fully conscious and myoclonic movements resolved completely. However, he continued to have his ear symptoms and underwent modified radical mastoidectomy. Histology showed granulation tissues. He was continued on ciprofloxacin and was discharged with advice to continue antibiotics for total duration of 3 months. There was no recurrence of myoclonus.
Myoclonus can occur as a side effect of multiple medications.[1] The mechanisms responsible for drug-induced myoclonus is not well understood.[2] Ceftazidime, is a third-generation cephalosporin widely used for the empiric treatment of infection in dialysis patients because of its broad antibacterial spectrum. But cautious adjustment in dosage is imperative for patients with renal insufficiency.[3] The mechanism of neurotoxicity and convulsions caused by cephalosporins involves the inhibition of γ-aminobutyric acid (GABA) binding to GABA receptors.[4] Impairment in active transport of cephalosporins from cerebrospinal fluid to blood due to competitive inhibition by accumulated toxic organic acids in patients with renal failure may account for the susceptibility to neurotoxicity.[5] Drug-induced myoclonus usually resolves after withdrawal of the offending drug. In this patient, the temporal association of the development of myoclonus after starting ceftazidime, and resolution following the discontinuation strongly suggests a causal relationship.
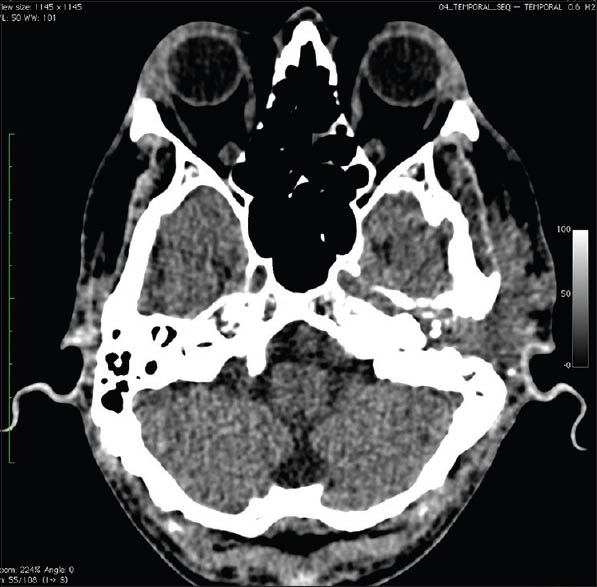
- Computed tomography scan skull showing extensive damage of left middle ear and ossicles
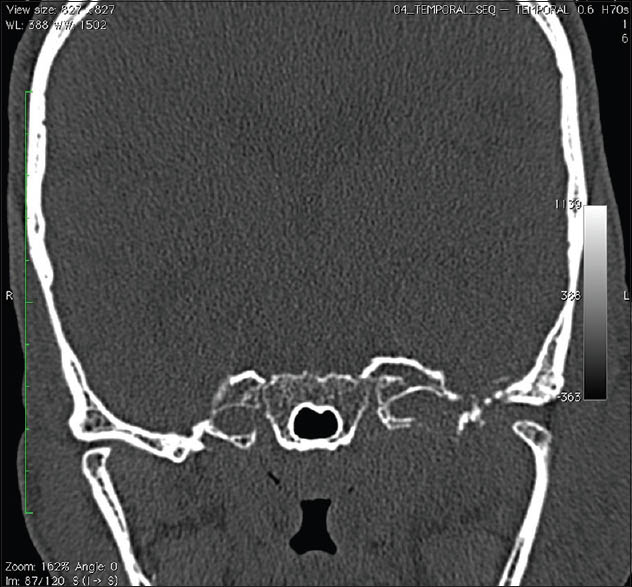
- Computed tomography skull coronal bone window showing skull base erosion
Due to the uncommon nature of the movement disorders induced by ceftazidime, which is commonly used in dialysis patients closer monitoring is advisable.
References
- Drug-induced myoclonus: Frequency, mechanisms and management. CNS Drugs. 2004;18:93-104.
- [Google Scholar]
- Neurotoxicity associated with ceftazidime therapy in geriatric patients with renal dysfunction. Pharmacotherapy. 1991;11:351-2.
- [Google Scholar]
- Evidence for the involvement of GABA (A) receptor blockade in convulsions induced by cephalosporins. Neuropharmacology. 2003;45:304-14.
- [Google Scholar]
- Drug intoxication and neurological episodes in chronic renal failure. Br Med J. 1970;2:394-5.
- [Google Scholar]




