

Translate this page into:
Antioxidant vitamins status in children and young adults undergoing dialysis: A single center study
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Vitamin E and C are well-known antioxidant vitamins. Oxidative stress is common in chronic kidney diseases. We evaluated 43 dialysis subjects prospectively in a cross-sectional survey. Serum vitamin E concentration was checked in all subjects; 37 cases underwent blood sampling for measurement of serum vitamin C. The enrolled subjects consisted of 12 (27.9%) peritoneal dialysis (PD) and 25 (58.1%) hemodialysis (HD) patients. Six (13.9%) patients were switched from PD to HD or vice versa. Serum concentration of vitamin E was normal, low and high in 9 (20.9%), 31 (72%) and 3 (7.1%) patients, respectively. There were no significant differences regarding age, gender, modality and duration of dialysis, and characteristics of dialysis sessions, mean serum blood urea nitrogen, and albumin levels between vitamin E deficient cases with those with normal serum vitamin E concentration (P > 0.05 for all). The serum vitamin C levels were low in 5 (13.5%) and normal in 32 (86.5%) patients. vitamin C deficiency was more prevalent in HD versus continuous ambulatory peritoneal dialysis patients (P = 0.128). Mean serum vitamin C concentration was higher in patients who were supplemented by vitamin C compared with those who didn’t receive the vitamin supplement (P = 0.043). Vitamin E deficiency was a prevalent finding and supplementary vitamin C 30–60 mg/day was sufficient to prevent deficiency. Regular assessments of serum vitamin E level may be needed in dialysis centers.
Keywords
Continuous ambulatory peritoneal dialysis
hemodialysis
Vitamin C
Vitamin E

Introduction
Free radicals are present in human cells as normal consequences of energy metabolism. Documented studies have shown oxidative damage to DNA, proteins and lipids by free radicals.[1] Vitamin E and C are two well-known antioxidant vitamins. Vitamin E has the ability to scavenge lipid radicals and terminate oxidative chain reactions.[2] Ascorbate represents one of the most prominent plasma as well as intracellular antioxidants with lipid peroxidation inhibitory effect by reducing endothelial dysfunction.[3] Ascorbic acid maintains copper and iron in a reduced state, and can act both as an antioxidant and a pro-oxidant.[4] Different in vivo and in vitro studies have performed to show anti-atherogenic effects of these antioxidants.[2]
Tissue hypoxia with oxidative stress is common in chronic kidney diseases (CKD). Hemodialysis (HD) however ameliorates hypoxia and lowers antioxidant vitamins levels.[5] Oxidative stresses during HD is attributable to peripheral blood mononuclear cells interaction with bio-incompatible dialysis devices, which results in increased synthesis and release of pro-inflammatory cytokines and imbalance between pro and antioxidant activities. These conditions may lead to complications, including cardiovascular disease, atherosclerosis, anemia and malnutrition.
New evidence suggests that dialysis patients have an impaired mitochondrial respiratory system, which may be the consequence or the cause of enhanced oxidative stress.[2] The aim of this study is defining antioxidant vitamins (Vitamin E and C) status in dialysis patients.
Materials and Methods
Forty-three dialysis patients, including 18 girls (41.9%) and 25 (58.1%) boys aged 19–300 (166 ± 76) months, who consented to participate in the study were enrolled. They included 12 (27.9%) patients who were placed on continuous ambulatory peritoneal dialysis (CAPD) and 25 (58.1%) HD subjects. Six (13.9%) patients during treatment were switched from peritoneal dialysis (PD) to HD or vice versa because of some complications related to dialysis modality (such as intractable peritonitis in PD cases, which needed catheter removal).
Serum vitamin E concentration was checked in all cases, and blood samples for measurement of serum vitamin C were obtained in 37 of 43 subjects. Blood samples for measuring serum vitamin E and C and routine monthly laboratory tests (serum blood urea nitrogen [BUN], creatinine, serum electrolytes, and complete blood count and serum albumin levels) were obtained at the time of the study. The serum BUN and hemoglobin (Hb) levels at the time of the study and serum levels in 1 and 2 months before the study, which were available in patient files, were used to calculate mean serum BUN and Hb levels. As serum albumin levels routinely were checked every 3 months in our subjects, the result of the last serum albumin levels (recent 3 months) were used in the study.
Clinical characteristics
The duration from onset of dialysis was 1–128 (44.3 ± 32.1) months. Vitamin C supplement was recommended routinely before or immediately after placing on dialysis, but unfortunately about half of cases stopped the vitamin consumption or used it irregularly. Eighteen patients were supplemented by vitamin C 30–60 (51.2) mg/day, whereas 11 and 14 subjects stopped consumption or were not sure about regular consumption, respectively. No vitamin E supplementation was recommended routinely.
The types of dialysis machines were Fresenius 4008 (Germany), AK95 and AK96 (Swiss) and the types of dialyzer were low flux (R3-R5 and low flux polysulfone membranes). The blood flow rates were regulated on 100–300 cc/min. The duration of dialysis session routinely was three 4-hour sessions per week, but a group of patients with severe volume overload symptoms were placed on four dialysis sessions per week and in some patients 3 h of dialysis in each session were recommended instead of a standard (4 h in each session) dialysis duration.
In CAPD group, the number of dialysis cycles per day was 4–6 (4.82 ± 0.52), with dwelling time of 2–4 (3.58 ± 0.71) h and dwelling solution volume of 27–77 (39.65 ± 16.14) cc/kg. The study was funded by a research grant from Mashhad University of Medical Sciences. Written consents were obtained from patients or their parents and the study was approved by local Ethic Committee.
Laboratory methods
Serum vitamin E and C levels were measured by HPLC.[67] For vitamin C values, 0.6–2 mg/dl was defined as normal, serum levels <0.6 mg/dl and >2 mg/dl were defined as low and high levels, respectively.
For vitamin E, the reference values of 3–9 μg/ml, 6–10 μg/ml and 5–18 μg/ml were defined normal values for children, teenagers and adult age groups, respectively. Values lower than 3 μg/ml, 6 μg/ml and 5 μg/ml in children, teenagers and adults were defined as vitamin E deficiency, respectively.
Blood samples in HD patients were obtained before dialysis sessions and during routine monthly sampling.
Statistical analysis
Descriptive statistics included mean values ± standard deviation (SD) for continuous and percentages for categorical data. Chi-square and independent t-tests were used for data analysis and P < 0.05 was considered as significant statistical differences. Univariate analysis was performed using a model with vitamin E and C as the dependent variables, and age, gender, modality, and duration of dialysis and characteristics of dialysis sessions (number of cycles/day, dwelling time and volume in CAPD patients and hours of dialysis per week in HD cases), mean serum BUN and albumin levels (as important nutritional indexes) as independent variables.
Results
Serum concentration of vitamin E was normal in 9 (20.9%), low in 31 (72%) and high in 3 (7.1%) patients. Serum levels ranged 0.6–20 (3.5 ± 4.1) μg/ml. Eight CAPD (25.8%), 21 HD (67.7%) and 2 (6.5%) patients who received both modalities had vitamin E deficiency. Serum vitamin E concentration was reported high in 1 HD and 2 cases that received both modalities [Table 1].

Comparing different independent variables in vitamin E deficient subjects with those who had normal serum vitamin E levels didn’t show any significant statistical differences (P > 0.05 for all) [Table 1].
Serum vitamin C levels were checked in 37 subjects and ranged 0.45–1.45 (0.92 ± 0.27) mg/dl. The serum levels were low in 5 (13.5%) and normal in 32 (86.5%) patients. All cases with vitamin C deficiency were HD patients [Table 2]. Vitamin C deficiency was more prevalent in HD versus CAPD patients (P = 0.128).

Mean serum vitamin C concentration in patients who were supplemented by vitamin C and those who didn’t receive vitamin C supplements were 1.04 ± 0.25 and 0.84 ± 0.23 mg/dl, respectively (P = 0.043) [Table 2].
In PD group, 7 cases were supplemented by vitamin C regularly, four had stopped the vitamin consumption and 1 patient was not sure about regular consumption. Vitamin C and E deficiencies were reported in 2 and 13 girls, respectively and 3 and 18 boys had low serum vitamin C and E concentration, respectively. Frequency of vitamin C and E deficiencies was as common in boys as in girls [Tables 1 and 2]. Combined vitamin E and C deficiencies were detected in 3 of 37 (8.3%) patients. All cases with combined vitamin E and C deficiencies were HD patients! Figures 1 and 2 present the ranges of serum vitamin E and C concentration changes according to dialysis modalities. Mean serum Hb levels (in recent 2 months) in patients with vitamin C deficiency (9.6 ± 2.96 mg/dl) were not significantly lower than those with normal serum vitamin C levels (10.62 ± 2.27 mg/dl) (P = 0.55).
Patients were followed for a 4-year period. During the follow-up, 11 patients (25.6%) died because of different complications of CKD. Of 31 patients with low serum vitamin E levels 8 cases died during follow-up, whereas in cases with normal serum vitamin E (9 patients) 3 died during follow-up (P = 0.175). Ten of 37 cases that underwent serum vitamin C measurement died during follow-up; all of them had normal serum vitamin C levels. Five subjects with low serum vitamin C levels were alive at final follow-up! (P = 0.143).
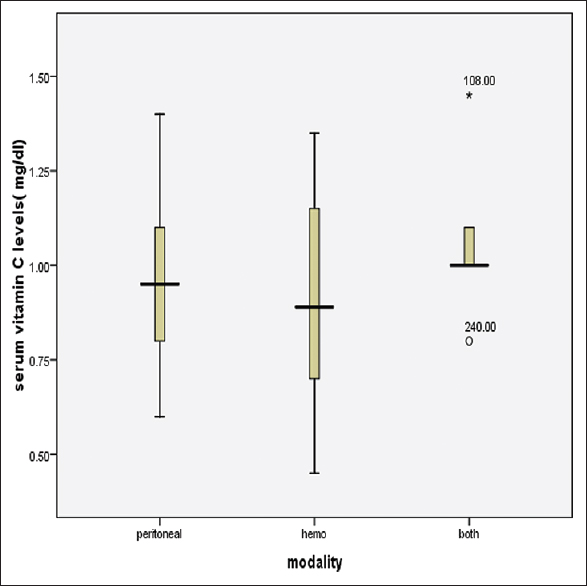
- Serum vitamin C concentration changes according to dialysis modalities
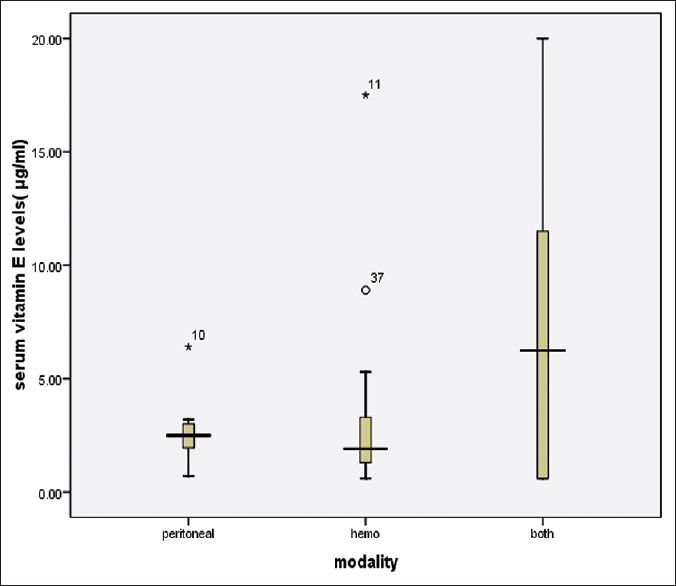
- Serum vitamin E concentration changes according to dialysis modalities
Discussion
Vitamin status depends on nutritional habits and lifestyle. Serum vitamin C concentrations depend on gender, age, smoking status, seasons, dietary intake and location of residence.[8] Ascorbic acid is involved in the formation and repair of collagen, development of bones and teeth, amino acid metabolism, synthesis of hormones, wound healing, and absorption and utilization of iron.[9] Adequate intake of vitamin E defined as per age ranged from 4 mg in infants younger than 6 months to 15 mg after the age of 14 years.[10] To avoid hyperkalemia, limiting the intake of potassium-rich foods especially in HD patients is recommended. As the major portion of dietary vitamin C is provided by potassium-rich foods, vitamin C deficiency has complicated the management of dialysis patients.[11] In addition, vitamin C metabolism results in oxalate production. To prevent oxalate accumulation in renal failure, vitamin C with a dose of 60–100 mg/day[11] or lower doses (50 mg)[12] is recommended that may not be optimal.[11]
The mean recommended dietary allowances (RDAs) for vitamin C is 65 and 75 mg/day for girls and boys, respectively.[13] Data from the US Department of Agriculture indicate that daily intake of vitamin C in age group 13 to 18 years olds is <30 mg in 14% of males and 20% of females.[14] Recent reports suggest that a dietary intake between 60 and 100 mg/day is sufficient to maintain adequate plasma vitamin C levels in subjects with normal kidney function.[4] Studies by the Renal Research Institute revealed that 15% of HD patients have vitamin C plasma levels <10 μmol/L, which indicates severe vitamin C deficiency[15] and is associated with scurvy.[16]
Zhang et al. assessed a large group of dialysis patients and noted vitamin C deficiency in about 1/3 of their cases.[16] In contrast to our findings they found vitamin C deficiency as common in HD as PD cases. A national health and nutrition examination survey by Hampl et al.[17] reported vitamin C deficiency among 5–17% and depletion in 13–23% of respondents. Dialytic vitamin C clearance, restricted intake of vitamin C-rich foods and increased vitamin C catabolism due to inflammatory process accounted for vitamin C deficiency as a common finding in dialysis patients.[4]
Approximately 10–25% of dialysis patients have vitamin C deficiency.[18] Vitamin C depletion during HD is substantial with plasma levels typically decreasing by 50% or more after a single dialysis treatment; this represents a dialytic removal of 100–300 mg of vitamin C depending on plasma levels,[1920] and Lower plasma levels of ascorbate in dialysis patients (who don’t receive supplementary vitamin) compared to healthy controls have been reported mainly due to a loss into the dialysate or increased urinary losses, so vitamin C supplementation 60 mg/day are recommended for CKD patients.[3]
Very high levels of vitamin C can also occur in dialysis patients. The normal kidney clears vitamin C when the plasma level exceeds 60 millimole (mM).[21] The lack of normal renal clearance mechanisms can result in very high plasma levels (>200 mM) in patients who take large amounts of vitamin C supplements.[22] Eighteen of our subjects were supplemented by 30–60 (51.2) mg/day vitamin C regularly. This range of the vitamin supplement resulted in normal serum concentration in all cases that were supplemented by vitamin C.
In contrast to our findings (no cases of vitamin C deficiency in PD patients), in a study by Lims et al.[23] although all of patients except one had total oral vitamin C intake above that of the US RDA (60 mg/day), 40% of CAPD patients had vitamin C deficiency. We found vitamin C deficiency in patients who either stopped the vitamin supplement consumption or their intakes were irregular. In contrast to our findings (no cases of vitamin C deficiency in PD patients), a wide range of plasma vitamin C levels, including both very low and high levels have been reported in dialysis patients.[1124252627]
It's suggested that normal serum vitamin levels are not good markers of deficiency, particularly for retinol,[28] vitamin E,[29] and C.[30] Vitamin C concentration in leukocytes is more reliable than simple serum concentrations for assessing tissue concentrations.[31] Like our series, Zhang et al.[32] reported that vitamin C deficiency is more common in HD than in PD patients. Yang et al.[33] suggested that intravenous vitamin C plus a vitamin E-coated dialyzer is effective in palliating oxidative stresses in HD patients.
Vitamin E is a powerful lipophilic chain-breaking antioxidant that delays lipid peroxidation. New functions of this antioxidant have been shown in polymorphonuclear leukocytes.[34] One study in Tunisia showed that 5.4% of school children have vitamin E deficiency (serum levels <6·97 μmol/l).[35]
Gentile et al.[36] recommended avoiding fat-soluble vitamin supplements (A and E) in dialysis patients and believed that their dietary intakes should be limited. Stein et al.[37] suggested that there is no need for vitamin E supplementation in dialysis patients, while Galli et al.[38] found relative vitamin E deficiency (low vitamin E/triglyceride ratio) in dialysis patients. They believed that vitamin E supplementation may be an effective therapy to combat oxidative stress in HD patients. Despite elevated plasma levels of vitamin E in dialysis patients, intracellular and clinical signs of hypovitaminosis are frequently found.[39] Cristol et al.[40] found abnormally low red blood cell vitamin E concentrations in dialysis patients.
Majority of our CAPD (66.7%) and HD (84%) patients had low serum vitamin E concentration. Neither characteristics of dialysis modalities (number of cycles, dwelling time and volume) in CAPD cases and hours of dialysis per week in HD patients or gender had any impact on the frequency of vitamin E deficiency in our series [Table 1]. Nutritional indexes such as serum BUN and albumin levels that were affected by amounts of protein intake were similar in vitamin E deficient group and patients with normal serum vitamin E concentration. As serum α-tocopherol is positively linked to the dietary intake, serum cholesterol and triglycerides,[8] it may be suggested that decreased fat intake is responsible for high incidence of vitamin E deficiency in our series. To determine the cause of vitamin E deficiency in our subjects, a study should be designed that focuses on the amounts of fat intake and the main dietary sources of vitamin E. Although it's reported that α-tocopherol is higher in males, whereas serum vitamin C is higher in females.[8]
Plasma vitamin C is positively associated with higher Hb level.[41] In our cases, mean serum Hb levels in patients with vitamin C deficiency were not lower than those with normal serum vitamin C levels.
Overall we noted that although first investigation in dialysis patients commonly reported high serum vitamin E concentration, it seems that vitamin E deficiency is not uncommon in dialysis subjects. What are the reasons for this trend of vitamin E deficiency in dialysis patients? Whether changes in dietary habits play any role is not clear and needs more investigations.
Results of our study showed that although literature review commonly suggested high serum vitamin E concentration in dialysis patients, it seems that vitamin E deficiency may be a prevalent finding in some dialysis centers and because of well-known antioxidant effects of vitamin E, serial screening for vitamin E deficiency in dialysis subjects should be considered especially in centers where vitamin E deficiency is a common finding. Overall, considering the cost-effectiveness of regular assessments of these vitamins, it needs to be determined whether measurement of vitamin E and C should be considered in patients on a regular dialysis? In addition, we found that supplementary vitamin C 30–60 mg/day is sufficient to prevent vitamin C deficiency in majority of patients and it also maintains the serum vitamin C concentration within normal ranges.
Higher prevalence of vitamin E and C deficiencies in HD compared to PD patients in our report is another positive point that adds to different advantages of PD modality. We didn’t find any significant differences in mortality rates between cases with vitamin E or C deficiency and those with normal levels of these vitamins.
The limitations of our study were low patient numbers, lack of nutritional status assessments and its effects on serum concentrations of vitamin E and C that should be emphasized by further studies.
Acknowledgment
The authors would like to appreciate Dr. Mohammad Esmaeeli, Dr. Fatemmeh Ghaneh and Dr. AbdolReza Varasteh for their advocated help.
Source of Support: Research and development section of Mashhad University of Medical Sciences
Conflict of Interest: None declared.
References
- Use of supplements of multivitamins, vitamin C, and vitamin E in relation to mortality. Am J Epidemiol. 2009;170:472-83.
- [Google Scholar]
- Mitochondrial dysregulation and oxidative stress in patients with chronic kidney disease. BMC Genomics. 2009;10:388.
- [Google Scholar]
- Vitamin C in chronic kidney disease and hemodialysis patients. Kidney Blood Press Res. 2003;26:100-6.
- [Google Scholar]
- Hypoxia and oxidative stress markers in pediatric patients undergoing hemodialysis: Cross section study. BMC Nephrol. 2012;13:136.
- [Google Scholar]
- Analysis of ascorbic acid and dehydroascorbic acid in biological samples. Methods Enzymol. 1999;299:65-76.
- [Google Scholar]
- Measurement of vitamin E in serum and plasma by high performance liquid chromatography with electrochemical detection. Ther Drug Monit. 1985;7:364-8.
- [Google Scholar]
- Factors influencing blood concentration of retinol, α-tocopherol, vitamin C, and β-carotene in the French participants of the SU.VI.MAX trial. Eur J Clin Nutr. 2006;60:706-17.
- [Google Scholar]
- Complete Book of vitamins and Minerals. Illinois: Publications International; 1993. p. :165-76.
- [Google Scholar]
- What is the recommended amount of vitamin E for children? Available from http://www.healthyeating.sfgate.com//
- [Google Scholar]
- Vitamin C deficiency in dialysis patients – are we perceiving the tip of an iceberg? Nephrol Dial Transplant. 2007;22:328-31.
- [Google Scholar]
- Nutritional status in dialysis patients: A European consensus. Nephrol Dial Transplant. 2002;17:563-72.
- [Google Scholar]
- Intakes of vitamin C, vegetables and fruits: Which schoolchildren are at risk? J Am Coll Nutr. 1999;18:582-90.
- [Google Scholar]
- Vitamin C deficiency and secondary hyperparathyroidism in chronic hemodialysis patients. Nephrol Dial Transplant. 2008;23:2058-63.
- [Google Scholar]
- Metabolism of 14C- and 3H-labeled L-ascorbic acid in human scurvy. Am J Clin Nutr. 1971;24:444-54.
- [Google Scholar]
- Low levels of vitamin C in dialysis patients is associated with decreased prealbumin and increased C-reactive protein. BMC Nephrol. 2011;12:18.
- [Google Scholar]
- Vitamin C deficiency and depletion in the United States: The Third National Health and Nutrition Examination Survey, 1988 to 1994. Am J Public Health. 2004;94:870-5.
- [Google Scholar]
- Effect of hemodialysis on total antioxidant capacity and serum antioxidants in patients with chronic renal failure. Clin Chem. 1995;41:1135-8.
- [Google Scholar]
- Vitamin C status of patients with chronic renal failure, dialysis patients and patients after renal transplantation. Int J Vitam Nutr Res. 1997;67:262-6.
- [Google Scholar]
- Convective and diffusive losses of vitamin C during haemodiafiltration session: A contributive factor to oxidative stress in haemodialysis patients. Nephrol Dial Transplant. 2002;17:422-7.
- [Google Scholar]
- Present Knowledge in Nutrition. (10th ed). Washington DC: ILSI Press; 1996. p. :146-59.
- [Google Scholar]
- The effect of vitamin C intake on plasma oxalate in patients on regular haemodialysis. Nephrol Dial Transplant. 1991;6:440-3.
- [Google Scholar]
- Oral intake and serum levels of ascorbic acid in continuous ambulatory peritoneal dialysis patients. Advances in Peritoneal Dialysis. 2001;17:215-8.
- [Google Scholar]
- Serum ascorbic acid and protein calorie malnutrition in continuous ambulatory peritoneal dialysis patients. Adv Perit Dial. 2001;17:219-22.
- [Google Scholar]
- Oral intake and serum levels of ascorbic acid in continuous ambulatory peritoneal dialysis patients. Adv Perit Dial. 2001;17:215-8.
- [Google Scholar]
- High prevalence of ascorbate deficiency in an Australian peritoneal dialysis population. Nephrology (Carlton). 2008;13:17-22.
- [Google Scholar]
- Vitamin C plasma level and response to erythropoietin in patients on maintenance hemodialysis. Nephrol Dial Transplant. 2004;19:2319-24.
- [Google Scholar]
- Vitamin E and relationships among tocopherols in human plasma, platelets, lymphocytes, and red blood cells. Am J Clin Nutr. 1988;47:470-4.
- [Google Scholar]
- Vitamin C: Prospective functional markers for defining optimal nutritional status. Proc Nutr Soc. 1999;58:469-76.
- [Google Scholar]
- Human requirements and needs. Vitamin C status: Methods and findings. Ann N Y Acad Sci. 1975;258:438-50.
- [Google Scholar]
- Association between vitamin C deficiency and dialysis modalities. Nephrology (Carlton). 2012;17:452-7.
- [Google Scholar]
- Effects of vitamin C infusion and vitamin E-coated membrane on hemodialysis-induced oxidative stress. Kidney Int. 2006;69:706-14.
- [Google Scholar]
- Monocyte superoxide production is highly sensitive and inversely related to normal changes of low density lipoprotein in alpha tocopherol. Atherosclerosis. 1998;138:263-9.
- [Google Scholar]
- Status of vitamins A and E in schoolchildren in the centre west of Tunisia: A population-based study. Public Health Nutr. 2011;14:255-60.
- [Google Scholar]
- Vitamin nutrition in patients with chronic renal failure and dietary manipulation. Contrib Nephrol. 1988;65:43-50.
- [Google Scholar]
- Vitamin levels in chronic renal failure and need for supplementation. Blood Purif. 1985;3:52-62.
- [Google Scholar]
- Vitamin E, lipid profile, and peroxidation in hemodialysis patients. Kidney Int Suppl. 2001;78:S148-54.
- [Google Scholar]
- True deficiency of antioxidant vitamins E and A in dialysis patients. Relationship with clinical patterns of atherosclerosis. Adv Perit Dial. 2002;18:206-11.
- [Google Scholar]
- Erythropoietin and oxidative stress in haemodialysis: Beneficial effects of vitamin E supplementation. Nephrol Dial Transplant. 1997;2:2312-7.
- [Google Scholar]
- Hemoglobin and plasma vitamin C levels in patients on peritoneal dialysis. Perit Dial Int. 2011;31:74-9.
- [Google Scholar]




