

Translate this page into:
Cytomegalovirus infection inducing flare of Behcet's disease with possible recurrence of glomerulonephritis after renal transplantation
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
We present a case of young male with end-stage renal disease due to type III membranoproliferative glomerulonephritis (GN) and clinical features consistent with Behcet's disease (BD). He developed flare of BD 3 months after deceased donor renal transplantation following cytomegalovirus infection, in the form of oral and genital ulcers. He also had GN characterized by mild mesangial proliferation, neutrophilic infiltration and subepithelial, mesangial and intramembranous electron dense deposits, which could possibly be attributed to recurrence of renal disease due to BD. The clinical flare of BD was treated with colchicine with good response.
Keywords
Behcet's disease
cytomegalovirus infection
renal transplantation

Introduction
Behcet's disease (BD) is a systemic vasculitis of unknown etiology involving small and large vessels, geographically mostly localized to regions of the ancient silk route. BD is characterized by recurrent oral aphthous ulcers, genital ulcers, uveitis, skin lesions and generally presents with remissions and exacerbations.[1] The clinical diagnosis of BD is generally done based on International Criteria for BD (ICBD) proposed in 2006.[2]
Renal involvement in BD is rare and generally mild. Reported incidence of renal disease in BD vary widely at 1–29%.[3] Akpolat et al. reviewed the published literature on renal disease in BD and found 253 cases.[3] AA-type amyloidosis was the major cause (43%) of renal disease in BD, followed by glomerulonephritis (GN) (35%) and renal micro or macrovascular disease (22%). A wide variety of histological patterns, such as diffuse proliferative GN, focal proliferative GN, focal segmental glomerulosclerosis, IgA nephropathy, membranoproliferative GN (MPGN), mesangial proliferative GN, membranous nephropathy and crescentic GN have been described in BD.[3] End-stage renal disease (ESRD) due to GN is very rare in BD and mostly it is due to AA-type amyloidosis or GN. In a survey of 331 dialysis centers across Turkey, Akpolat et al. reported only 7 cases of BD among 20,596 dialysis patients (0.07%).[4] The disease activity appeared quiescent in them, indicating that uremia or dialysis has a disease modifying effect.
We report a case of BD in a young male who had flare of the disease 3 months after renal transplantation following cytomegalovirus (CMV) infection that was characterized by oral aphthous ulcers, genital ulcer and GN.
Case Report
A 25-year-old male presented in 2009 at another hospital with headache and was detected to have moderate renal failure (serum creatinine [SCr]: 3.6 mg/dl). He underwent renal biopsy in November 2009, which showed 9 glomeruli, of which 4 showed ischemic sclerosis. The viable glomeruli showed lobulation of tuft, capillary wall splitting and thickening with mesangial interposition. There was mild tubular atrophy, dense interstitial round cell infiltrates with many collections of foam cells. Immunofluorescence showed focal peripheral and abundant mesangial granular C3c and IgM deposits. Renal biopsy showed features consistent with membranoproliferative GN type III. He resorted to indigenous medication and did not consult a physician. During this period, he had few episodes of oral aphthous ulcers that healed spontaneously.
He presented to us with uremic symptoms in December 2010 and was found to have severe azotemia (SCr: 8.9 mg/dl) and was initiated on hemodialysis. His urine analysis at that time showed 2+ albuminuria and red blood cells (RBCs) 2/hpf. He underwent hemodialysis thrice a week. He developed redness of eye in February 2011 during an episode of urinary tract infection that subsided spontaneously.
He received a deceased donor renal transplantation on July 14, 2012. The donor was a 19-year-old male, a victim of road traffic accident. He was given induction immunosuppression with intravenous basiliximab and triple immunosuppression in the form of cyclosporine, mycophenolate, and prednisolone. He had slow recovery of renal function after transplantation, but did not require dialysis. The serum creatinine was 2.6 mg/dl 1-week after transplantation. One month after transplantation, his blood pressure was 110/80 mm Hg without any antihypertensive drugs and allograft function was good (SCr: 1.2 mg/dl). Cyclosporine trough level was 142 ng/ml and ultrasonography showed normal allograft. Urine examination showed nil albumin and 14–16 RBCs/hpf. At this time, the immunosuppression consisted of prednisolone 10 mg, mycophenolate mofetil sodium (MMF-sodium) 360 mg twice daily and cyclosporine neoral 100 mg twice daily (4 mg/kg/day). He was given valganciclovir 450 mg daily for 8 weeks and cotrimoxazole prophylaxis. Cyclosporin trough level varied from 142 to 245 ng/ml. On September 15, 2012, he reported oral aphthous ulcer that was treated with multivitamin supplements and it resolved spontaneously within 10 days. At 3 months (October 5, 2012), he developed low-grade fever and mild increase in SCr from 1.2 to 1.4 mg/dl. CMV PP65 antigen was positive (46 × 2/105) and CMV polymerase chain reaction (PCR) was positive (205 copies/ml). He was initiated on intravenous ganciclovir 250 mg daily. He was admitted to the hospital 10 days later with gross hematuria, but no fever. Urine culture grew Klebsilla, which was treated with appropriate antibiotic. Urine examination showed plenty of RBCs and 2+ albuminuria and 24-h urine protein was 5.3 g/day. While on ganciclovir, he developed neutropenia and hence, the drug was stopped after 14 days, following which CMV PCR was negative. Following CMV activation, MMF-sodium was replaced by azathioprine 100 mg daily. During this period, he had recurrence of oral ulcers and a large genital ulcer [Figure 1] which was apparently present for few days prior to reporting to us. Tzanck smear of oral ulcer was negative for viral inclusions. Gross hematuria improved spontaneously, but microscopic hematuria persisted and SCr improved to 1.2 mg/dl spontaneously and he was discharged on prednisolone 10 mg daily, cyclosporin neoral 100 mg twice daily and azoran 75 mg daily. Despite above therapy, the oral and genital ulcers were persistent. About 2 weeks after discharge, on November 9, 2012, SCr increased to 1.6 mg/dl and a renal allograft biopsy was done. Renal biopsy showed 3 glomeruli with increased mesangial matrix and cellularity with focal infiltration of the tuft with few neutrophils [Figure 2]. The basement membrane (BM) was thin; there were mild patchy mononuclear cell infiltration with no significant tubulitis. Some tubules showed microcalcific deposits in the lumina. No viral inclusions were seen on the biopsy. Immunofluorescence study showed abundant peripheral and mesangial deposits of C3c [Figure 2] and mild deposit of IgM in the glomeruli and C4d stain was negative. The final conclusion was neutrophilic glomerulitis, mesangial proliferation and mild patchy interstitial mononuclear cell infiltrates with acute tubular necrosis. The electron microscopy study of renal tissue showed patent glomerular capillary loops with mild mesangial expansion and uniform BM. There were a few medium to large hump-shaped electron dense deposits in the subepithelium, mesangium with occasional intramembranous deposits. No subendothelial electron dense deposits were seen, and there was no area of new BM formation.
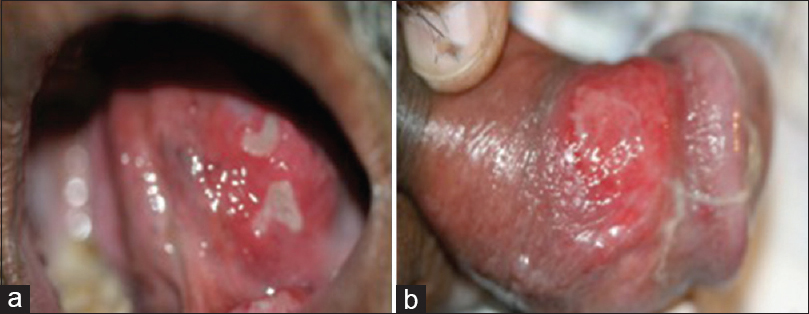
- Mucosal ulcers. (a) oral mucosal aphthous ulcers, (b) penile ulcer
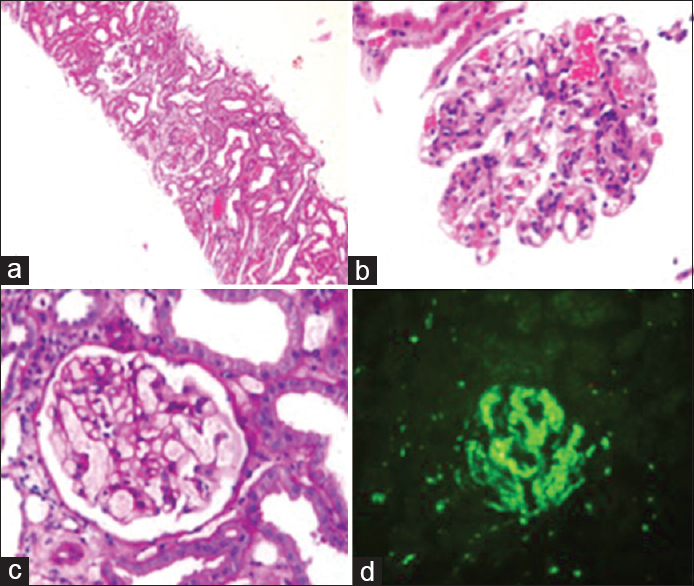
- Photomicrograph of renal biopsy. (a) light microscopy, (b and c) glomerulus showing mesangial proliferation and neutrophilic infiltrates, (d) immunofluorescence showing abundant peripheral and mesangial C3 deposits
Serum complement C3 was low at <16.9 mg/dl (normal 80–156 mg/dl) and serum C4 was normal. Antineutrophil cytoplasmic antibody was negative. Urine for BK virus was negative by PCR. He underwent biopsy of the oral ulcer, which showed subepithelial vascular proliferation, and perivascular lymphocytic infiltration along with scattered neutrophils, consistent with vasculitis [Figure 3]. He was diagnosed to have BD based on ICBD and histology of the oral ulcer. He was started on colchicine 0.5 mg twice daily, and cyclosporin was replaced by tacrolimus due to interaction between colchicine and cyclosporin. Following this treatment, his condition improved remarkably and oral and genital ulcers healed over 2 weeks. GN in our patient occurred along with a clinical flare of BD triggered by CMV infection and was thought to be a renal manifestation of BD. Subsequently, he did well and 15 months after transplantation SCr was 1.1 mg/dl (modification of diet in renal disease [MDRD] glomerular filtration rate 80 ml/min) and had proteinuria of 3.25 g/day and mild microhematuria. At this point, he received prednisolone 7.5 mg, tacrolimus 2.5 mg twice daily, azathioprine 75 and 100 mg on alternate days, enalapril 10 mg twice daily, colchicine 0.5 mg 3 times daily, omega-3 fatty acid 300 mg 3 times daily. Tacrolimus trough level was maintained at 4.0–5.0 ng/ml.
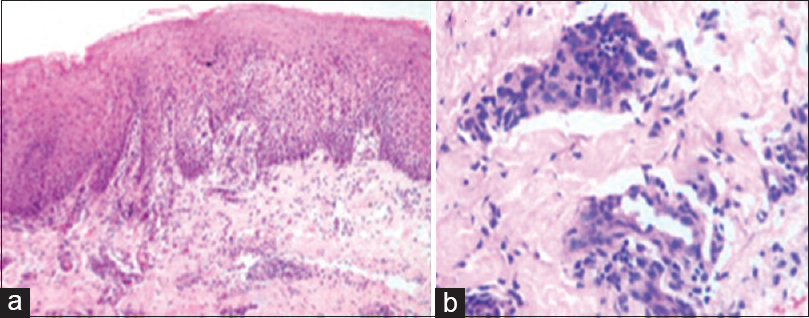
- Photomicrograph of the mucosal ulcer. (a) light microscopy showing subepithelial vascular proliferation, (b) perivascular lymphocytic infiltration with scattered neutrophilic infiltrates
Discussion
Diagnosis of BD was missed in our patient prior to the renal transplantation though clinical features of the disease were evident. This may be due to the fact that BD is very rare in Southern India, and the awareness of the disease is poor amongst the clinicians. The flare of BD after renal transplantation was characterized by recurrent nonhealing oral aphthous ulcers and genital ulcer. The Tzanck smear was negative for viral inclusions. The patient fulfilled 5 out of 7 clinical criteria proposed by the ICBD.[2] The histology of oral ulcer biopsy was consistent with vasculitis due to BD. Oral and genital ulcer did not heal despite adequate treatment of CMV infection with valganciclovir but resolved rapidly following treatment with colchicine, which supported the diagnosis of BD.[5]
Very few cases of successful renal transplantation in patients with BD have been reported in the literature,[67] but recurrence of GN in allograft has not been reported previously. Lai et al. reported BD presenting as colonic ulcer in a renal transplant recipient, however, this patient did not have BD prior to transplantation.[8] Our patient had mild mesangial proliferative GN with glomerular neutrophilic infiltrates, presenting with nephrotic range proteinuria and hematuria, mild azotemia and low levels of complement C3. The EM study revealed mesangial, intramembranous and subepithelial electron dense deposits. This picture is consistent with early MPGN type III, which is similar to the histology seen in native kidney. Similar histological pattern of injury may be seen in postinfectious GN (PIGN) and CMV glomerulopathy. However, there was no evidence of any infection other than CMV infection in our patient, and hence PIGN was excluded. CMV glomerulopathy is a controversial lesion. CMV glomerulopathy is characterized by significant interstitial inflammation (62% cases), glomerular thrombi (20%), CMV inclusion bodies (20%) and glomerular neutrophil infiltration (15%).[9] Our case did not have significant interstitial inflammation, nor CMV inclusions and had mild neutrophilic infiltration, which argue against the CMV glomerulopathy. Moreover, the CMV activity based on viral replication by PCR was mild, and GN did not improve following the successful treatment of CMV infection with valganciclovir. Clinical improvement of glomerular disease coincided with a resolution of symptoms of BD following treatment with colchicine. These observations support our belief that GN after renal transplantation was a part of the renal manifestation of BD and constituted recurrence of the disease in allograft. However, despite some evidence in support of BD induced GN, we cannot categorically exclude the possibility of PIGN such as that induced by CMV infection in our patient.
The etiology of BD remains unknown, but epidemiologic findings suggest that an autoimmune process is triggered by an infectious or environmental agent in a genetically predisposed individual in BD.[10] Most explored are the infective agents especially viruses in the etiopathogenesis of BD; several viruses such as herpes simplex virus and CMV have been implicated, but conclusive evidence is lacking.[10] Martín et al. reported a flare of BD following CMV infection indicating a possible pathogenic role of CMV.[11] A clear association of clinical flare of BD and CMV infection was noted in our patient, which strongly support the hypothesis that CMV infection is involved triggering clinical flare of BD.
Conclusions
We present a young male suffering from BD, who reached ESRD due to the progression of type III MPGN and required a renal transplantation. After renal transplantation he acquired CMV infection that caused flare of BD, which manifested in the form of oral and genital ulcers and GN. There was a significant improvement in BD following treatment with colchicine with healing of ulcers and improvement in GN.
Source of Support: Nil
Conflict of Interest: None declared.
References
- International Team for the Revision of the International Criteria for Behcet's Disease. Evaluation of the International Criteria for Behcet's disease (ICBD) Clin Exp Rheumatol. 2006;24(Suppl 42):S13.
- [Google Scholar]
- Colchicine versus placebo in Behçet's disease: Randomized, double-blind, controlled crossover trial. Mod Rheumatol. 2009;19:542-9.
- [Google Scholar]
- A successful renal transplantation in Behçet's syndrome. Ann Rheum Dis. 1999;58:719.
- [Google Scholar]
- Renal transplantation in a C-ANCA(+) patient with Behcet disease and rapidly progressive glomerulonephritis. Clin Nephrol. 2004;61:357-9.
- [Google Scholar]
- Recurrent oral ulcers and diarrhea in a renal transplant patient. Behcet's disease (associated with IgA nephropathy) and acute tacrolimus nephrotoxicity. Kidney Int. 2009;76:1211-2.
- [Google Scholar]
- CMV infection of the renal allograft is much more common than the pathology indicates: A retrospective analysis of qualitative and quantitative buffy coat CMV-PCR, renal biopsy pathology and tissue CMV-PCR. Nephrol Dial Transplant. 2003;18:397-402.
- [Google Scholar]
- Potential Infectious Etiology of Behçet's Disease. Patholog Res Int 2012 2012:595380.
- [Google Scholar]
- Severe flare of Behcet's disease with intense mucucutaneous manifestations. Reumatol Clin. 2010;6:303-5.
- [Google Scholar]




