

Translate this page into:
End-stage renal disease in Tunisian infants: Etiology and outcome
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
End stage renal disease (ESRD) in infants has particular features in terms of etiologies and therapeutic modalities. The aim of our study is to describe the etiologies and the ESRD outcomes among Tunisian infants. This retrospective study was conducted over 15 years (from January 1998 to December 31, 2013) in the Pediatric Department at Charles Nicolle Hospital. In total, 157 pediatric patients had ESRD. The mean incidence was 4.25 million children. The study involved 24 infants; the sex ratio was equal to 2. The mean age at diagnosis of ESRD was 8 months (range, 1–21 months). Growth retardation was noticed in 14 patients. The main causes were Congenital Anomalies of the Kidneys and Urinary Tract (9 infants) and hereditary renal disease (9 infants). All patients were treated with peritoneal dialysis; 16 infants presented peritonitis. Mortality rate was about 28%. The leading causes of death were cardiovascular diseases and infections.
Keywords
Dialysis
end-stage renal disease
infant
mortality

Introduction
End stage renal disease (ESRD) is a serious health problem among children, especially among children aged <2 years. It has particular features in terms of etiology and therapeutic modalities.[12] The management of infants with ESRD aims, on the one hand, at increasing patients’ longevity and, on the other hand, at improving growth and life-quality.[34]
ESRD incidence among children is estimated at 5.5 new cases per million inhabitants per year in Europe, 10.6[5] in Canada, and 4[6] in Japan.[78] In developed countries, prognosis of pediatric ESRD has improved; most children can have access to chronic peritoneal dialysis (PD), Hemodialysis, or kidney transplantation. Conversely, in developing countries, ESRD is a serious cause of morbidity and mortality. Managing ESRD is particularly challenging due to patients late presentation, poor socioeconomic conditions, and inadequate health care infrastructure support. Data from developing countries are rare. Some data found in Nigerian series report an incidence of 4 cases/million inhabitants per year.[910]
In Tunisia, a single epidemiological study, in 1993, examined the ESRD epidemiological aspects,[11] since then no data about ERSD among infants has ever been collected. The aim of our study was to describe ESRD etiologies and outcomes among Tunisian infants.
Methods
This retrospective study included all infants with the ESRD diagnosis who presented to the Department of Pediatric Nephrology at Charles Nicolle Hospital in Tunis from January 1998 to December 2013. ESRD patients were defined as those who needed renal replacement therapy (RRT) to sustain life. We excluded foreign-born patients, those whose death occurred within a short time. Individual patient data included date of birth, gender, primary renal disease, starting RRT date, treatment modality at start of RRT, and important events such as death. Demographic data were collected from the National Statistics Institute records.
Results
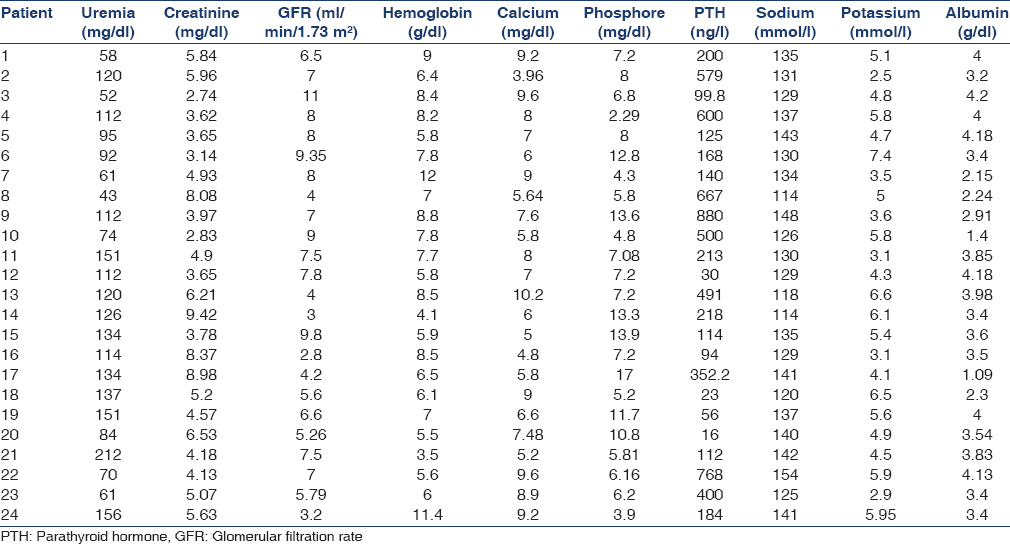
We studied 157 children with ESRD who were treated in the Pediatric Department at Charles Nicolle Hospital. The mean incidence was 4.25 cases/million children aged <15 years. 24 children (15.2%) were infants; the sex ratio was equal to 2. The mean age of infants with ESRD at presentation was 8 months (range, 1–21 months). Consanguinity was found in 58% of the infants. A family history of chronic kidney disease was noticed in 8.3% of the infants. Growth retardation was observed in 54% of the patients. Laboratory findings were as follows: mean serum creatinine: 5.6 (3.1–9) mg/dl, mean blood urea nitrogen: 95 (18–243) mg/dl, and hemoglobin: 6 (3.5–12) g/dl. Hyponatremia was observed in 10 infants. Hypocalcemia was noticed in 13 infants and hyperphosphatemia in 20 infants [Table 1].
The main causes were congenital anomalies of the kidneys and urinary tract (CAKUT) (9 infants), inherited renal disease (9 infants), hemolytic and uremic syndrome (3 cases), and unknown origin (3 cases). Seventeen infants were treated with erythropoietin, and 9 infants received growth hormone. None of our patients had a feeding gastrostomy. All patients were treated by PD, all infants had double-cuff straight Tenckhoff catheter, 20 infants were treated with continuous ambulatory PD and 4 infants with automated PD; 17 infants had peritonitis. Mean follow-up time was 41.3 months (range, 1–210 months). The mortality rate was 28%. The leading death causes were cardiovascular diseases and infections.
Discussion
This study presents ESRD etiology and outcome among Tunisian infants. To the best of our knowledge, none of the studies have so far focused exclusively on infants with ESRD and, therefore, our study adds new insights to ESRD etiologies and outcome among Tunisian infants. ERSD is rare in infants. It has particular characteristics in terms of etiology and therapeutic modalities. Over the last few years, an increasing pediatric ESRD incidence has been observed in Europe and North America.[51213] The rising incidence of RRT was attributed to the increase of dialysis provision to younger children by virtue of improvements in techniques for nutritional and dialysis support.
The male predominance noted in this study is similar to observations in many other reports. As in the other studies,[121314] male predominance is due to the higher proportion of males among patients with CAKUT.
In our series, growth retardation was noticed in 14 patients, but only 9 patients received growth hormone. None of our patients had a feeding gastrostomy. This is explained by poor socioeconomic conditions and expensive treatments.
In our study, CAKUT and inherited renal disease account for the majority of ESRD cases. Hemolytic uremic syndrome contributes to a lesser extent. Reports from Europe,[12] Australia,[12] Japan,[8] Kuwait,[15] Turkey,[16] and the United States[13] show that CAKUT are the leading causes of ESRD and are responsible for between 34% and 52% of ESRD cases among children; ESRD in younger children is mostly due to CAKUT. The high prevalence of inherited renal disease among infants in our study is attributed to the high proportion of consanguinity (58%). Environmental, ethnic, and other differences might explain the different occurrences of primary renal diseases in Europe and in other parts of the world as compared with our findings.
Access to chronic RRT has improved the ESRD outcome in developed countries.[51314] A Tunisian research dated 1997[11] found that the therapeutic abstention rate attained 19%. In our study, all infants received RRT. PD was the treatment modality employed for all patients. The major complication in our series was peritonitis. A Korean study[17] reported a frequency equal to 21.7% of peritonitis among infants undergoing PD. A British study[18] published in 2010 reported that the peritonitis incidence was estimated at 66.66%.
Long-term survival rate for children with chronic RRT in developed countries is 79% at 10 years and 66% at 20 years.[1920] However, within the Nigerian study, mortality affects 59% of children with ESRD.[9] The mortality rate in our study was high. Major death causes identified in this study were infections, followed by cardiovascular causes as is reported in the literature.[51920]
Conclusion
In Tunisia, management of children with ESRD has known progress in recent years; yet, mortality rate in infants with ESRD is high. The current high rate of mortality can be improved by earlier referral, better nutrition, family support, and enhanced access to treatment modalities.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Chronic kidney disease in children: The global perspective. Pediatr Nephrol. 2007;22:1999-2009.
- [Google Scholar]
- Renal replacement therapy in children: Data from 12 registries in Europe. Pediatr Nephrol. 2004;19:213-21.
- [Google Scholar]
- Estimated prevalence of childhood end-stage renal disease in the state of São Paulo. Rev Assoc Med Bras. 2011;57:436-41.
- [Google Scholar]
- Long-term survival of children with end-stage renal disease. N Engl J Med. 2004;350:2654-62.
- [Google Scholar]
- Demographics of paediatric renal replacement therapy in Europe: A report of the ESPN/ERA-EDTA registry. Pediatr Nephrol. 2014;29:2403-10.
- [Google Scholar]
- Disparities in treatment rates of paediatric end-stage renal disease across Europe: Insights from the ESPN/ERA-EDTA registry. Nephrol Dial Transplant. 2015;30:1377-85.
- [Google Scholar]
- Canadian Institute for Health Information, Health Services Databases. Available from: http://www.cihi.ca
- Progression to end-stage kidney disease in Japanese children with chronic kidney disease: Results of a nationwide prospective cohort study. Nephrol Dial Transplant. 2014;29:878-84.
- [Google Scholar]
- Paediatric end-stage renal disease in a tertiary hospital in South West Nigeria. BMC Nephrol. 2014;15:25.
- [Google Scholar]
- The management of end-stage renal disease in underdeveloped countries: A moral and an economic problem. Pediatr Nephrol. 1990;4:199-201.
- [Google Scholar]
- End-stage renal disease of the Tunisian child: Epidemiology, etiologies, and outcome. Pediatr Nephrol. 1996;10:479-82.
- [Google Scholar]
- ANZDATA Registry. Report Downloads Area. Available from: http://www.anzdata.org.au/v1/report.html
- 2010. U.S Renal Data System: USRDS 2010 Annual Data Report: Atlas of end stage End-Stage Renal Disease in the United States, 2010. Bethesda, MD: National Institute of Health, National Institute of Diabetes and Digestive and Kidney Diseases; Available from: http://www.usrds.org/adr.aspx
- End-stage renal disease in Slovak children: Epidemiology from a European perspective. Eur J Pediatr. 2011;170:1445-51.
- [Google Scholar]
- End-stage renal disease in Kuwaiti children: An 8-year experience. Transplant Proc. 2004;36:1788-91.
- [Google Scholar]
- Chronic peritoneal dialysis in Turkish children: A multicenter study. Pediatr Nephrol. 2005;20:644-51.
- [Google Scholar]
- Outcomes of peritonitis in children on peritoneal dialysis: A 25-year experience at Severance Hospital. Yonsei Med J. 2013;54:983-9.
- [Google Scholar]
- Peritonitis in children on chronic peritoneal dialysis; experience from a paediatric nephrology centre. Arch Dis Child. 2010;95:83-4.
- [Google Scholar]
- Etiology and epidemiology of end-stage renal disease in Dutch children 1987-2001. Pediatr Nephrol. 2005;20:1136-42.
- [Google Scholar]
- Long-term outcomes of children with end-stage renal disease. Pediatr Nephrol. 2005;20:849-53.
- [Google Scholar]




