

Translate this page into:
An unusual case of gastrointestinal mucormycosis in a patient with nephrotic syndrome
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Immunosuppression predisposes to a variety of infections, some of which occur at unusual sites. Of all the forms of mucormycosis, involvement of the intestines is rare. High degree of suspicion along with the use of invasive procedures can facilitate the diagnosis of these infections. We report a rare case of gastrointestinal Mucor in a patient with nephrotic syndrome.
Keywords
Gastrointestinal Mucor
immunosuppression
nephrotic syndrome
unusual infection

Introduction
Mucormycosis is a serious infection due to fungi of the order mucorales. Immunosuppressed states predispose to this fatal condition. Rhino cerebral form is the most common presentation of this infection followed by lung involvement. Gastrointestinal (GI) mucormycosis is a relatively rare manifestation seen in 7% of cases.[1]
We report a patient with nephrotic syndrome whose course was complicated by gastrointestinal Mucor.
Case Report
A 45-year-old male, hypertensive for 2 years, nondiabetic, nonsmoker, and teetotaler, presented with a history of swelling of both lower limbs and face of 4 weeks duration and low-grade fever with melena of 10 days duration. There was no history of pain abdomen, diarrhea, hematochezia, vomiting, abdominal distention, cough, oliguria, dysuria, or pyuria.
Past history was significant for biopsy-proven membranous nephropathy a year ago. His 24 h urine protein was 10 g and serum creatinine was 1 mg/dl at that time. He received modified Ponticelli regimen consisting of alternate steroids (0.5 mg/kg/day and cyclophosphamide (2 mg/kg/day) for 6 months. His symptoms subsided after 4 months of completing the therapy but attained only partial remission with 24 h protein of 2 g. He was continued on tablet losartan 50 mg and tablet atorvastatin 10 mg. There was no history of tuberculosis in the past. There was a history of pains in both knees for which he was taking over the counter nonsteroidal anti-inflammatory drugs and oral steroids intermittently for 2 years prior to these symptoms.
On admission, he was conscious and coherent with pallor and generalized edema. Investigations revealed hemoglobin of 5 g/dl, total leukocyte count of 29,900/mcl with >90% polymorphs and normal platelet counts. Urine examination revealed 4 + albumin with 10–12 red blood cell/hpf and plenty of pus cells. Serum creatinine was 4.5 mg/dl. Serum electrolytes and liver enzymes were normal. Serum proteins and serum albumin were 3.6 and 1.5 g/dl, respectively. Coagulation parameters were within normal limits. Twenty-four-hour urine protein was 8.2 g. Blood and urine cultures were sterile. Blood transfusions were given with two packed cells. Stool for occult blood was positive. Iron profile revealed transferrin saturation of 18% with serum ferritin of 200 mcg/l. Serum vitamin B 12 and folate levels were normal. In view of melena and blood in stools, colonoscopy was done which revealed a large ulcer in proximal ascending colon near cecum. Rest of the colonic mucosa was normal. Upper GI endoscopy was normal. Biopsy was taken from ulcer site.
Histopathology revealed numerous fungal hyphae with necrosis on PAS stain, as shown in the block area of the figure [Figure 1]. High-power view showed thick-walled, aseptate, obtuse-angled branching hyphae [Figure 2]. Silver methenamine stain highlighted the fungal elements in black colour [Figure 3]. The picture was suggestive of Mucormycosis.

- Central necrosis (block area) with surrounding numerous fungal hyphae with PAS stain
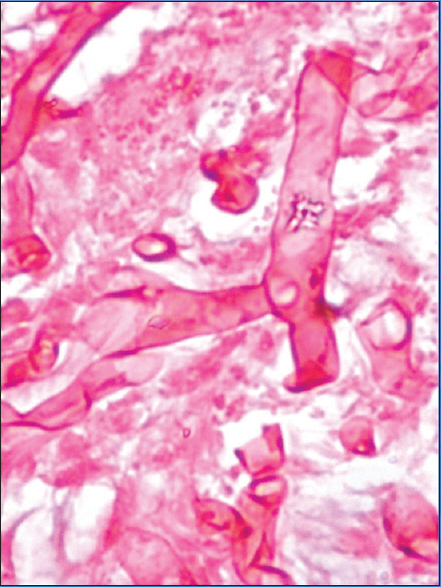
- Thick-walled, aseptate, obtuse-angled branching hyphae on high power view with PAS stain

- Fungal elements in black colour with Silver methenamine stain
The patient was started on intravenous amphotericin B 1 mg/kg/day. The conventional formulation was used instead of liposomal form due to financial constraints. No surgical debridement was done due to well-preserved general condition of the patient. A total dose of 2.8 g of drug was given. Repeat colonoscopy revealed a healing ulcer. Further administration of amphotericin B was stopped. Patient was started on losartan 50 mg and atorvastatin 20 mg. He was on follow-up with us on OPD basis with a serum creatinine of 2.6 mg/dl and stable general condition. His 24 h urine protein was 4 g and he is being continued on same drugs. He did not receive any further immunosuppressive medications.
Discussion
Mucormycosis is a life-threatening infection caused by fungi of the subphylum mucoromycotina, order mucorales.[2]
The infection is highly invasive and relentlessly progressive with high morbidity and mortality (>40%). Risk factors for the development of this disease include immunosuppressed states such as posttransplant, both solid organ and stem cell transplant patients, diabetics, neutropenia, and people with excess iron stores.[345]
These fungi are ubiquitous and humans are constantly exposed to them. Oral consumption of spores through food or water source leads to gastrointestinal manifestations, which can be complicated by perforation of viscera. More than eighty publications of gastrointestinal mucormycosis exist till 2012.[6] In Indian literature, Chakrabarti et al. reported 178 cases of Mucormycosis of which GI involvement was documented in 8.4%.[7] From our institute, first case report dated to 2006, when we presented a postrenal transplant patient with gastric mucormycosis and co-existent strongyloidiasis.[8]
The most common gastrointestinal site of involvement is stomach, followed by colon and ileum.[9] Majority of the previous case reports were in premature infants who acquired the disease as a part of disseminated disease. Recent reviews identified the disease in immunocompromised patients as in HIV and posttransplant patients. Presenting symptoms include nonspecific abdominal pain, nausea, and vomiting with GI bleed.
More than 50% of cases are diagnosed postmortem. The most specific and sensitive modality to diagnose this condition is a histopathological examination of the involved tissue. Characteristic appearance includes wide (6–30 µm), thick-walled, ribbon-like, aseptate hyphal elements that branch at right angles. These are best visualized with PAS stain. Culture, though less sensitive, is very effective for identifying the underlying species. An invasive procedure like endoscopy and bronchoscopy is often required in many cases for tissue diagnosis. A high index of suspicion is required to diagnose this condition.
In our case, the use of immunosuppressive therapy in the form of Ponticelli regimen, along with over-the-counter oral steroids, might have predisposed the patient to this infection. Nephrotic syndrome itself was another contributing factor for the infection. Only with invasive procedure in the form of colonoscopy and tissue biopsy, we were able to identify etiology of the ulcer. In fact, only 25% cases of gastrointestinal disease are diagnosed antemortem.
Untreated case of GI mucormycosis has high mortality rates of >80%. Definitive management involves surgical resection of the lesion and early initiation of polyene antibiotics, for example, amphotericin B. Posaconazole has shown in vitro activity against mucorales. Combination therapy with echinocandins and polyene antibiotics has shown superiority in some mice studies and in a small case series of rhino-cerebral mucormycosis patients. In our patient, surgical resection was withheld in view of improving general condition of the patient.
Conclusion
Mucormycosis is a life-threatening infection with varied presentations. Isolated gastrointestinal involvement is rare. High degree of clinical suspicion is required to diagnose this condition often necessitating the use of invasive procedures for demonstration of the fungus. Definitive treatment involves early initiation of antifungals with or without surgical resection of the lesion.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- A higher-level phylogenetic classification of the Fungi. Mycol Res. 2007;111(Pt 5):509-47.
- [Google Scholar]
- Epidemiology and outcome of zygomycosis: A review of 929 reported cases. Clin Infect Dis. 2005;41:634-53.
- [Google Scholar]
- Recent advances in the management of mucormycosis: From bench to bedside. Clin Infect Dis. 2009;48:1743-51.
- [Google Scholar]
- Novel perspectives on mucormycosis: Pathophysiology, presentation, and management. Clin Microbiol Rev. 2005;18:556-69.
- [Google Scholar]
- Gastrointestinal mucormycosis: An evolving disease. Gastroenterol Hepatol (N Y). 2012;8:140-2.
- [Google Scholar]
- The rising trend of invasive zygomycosis in patients with uncontrolled diabetes mellitus. Med Mycol. 2006;44:335-42.
- [Google Scholar]
- Non-fatal gastric mucormycosis in a renal transplant patient and review of the literature. Transpl Infect Dis. 2006;8:237-41.
- [Google Scholar]
- CT and sonographically guided biopsy in a patient with intestinal mucormycosis. AJR Am J Roentgenol. 2000;175:129-31.
- [Google Scholar]




