

Translate this page into:
A Case of Infected Renal Cyst Complicated by Renal Vein Thrombosis
Corresponding author: Prof. Dong J. Park, Department of Internal Medicine, Gyeongsang National University Changwon Hospital and Gyeongsang National University College of Medicine, 11 Samjungja-ro Sungsan-gu, Changwon, 51472, Republic of Korea. E-mail: drpdj@naver.com
-
Received: ,
Accepted: ,
How to cite this article: Ryu J, Lee S, Lee TW, Bae E, Park DJ. A Case of Infected Renal Cyst Complicated by Renal Vein Thrombosis. Indian J Nephrol. 2024;34:265–7. doi: 10.4103/ijn.ijn_289_23
Abstract
Renal vein thrombosis (RVT) is not an uncommon condition in patients occurring nephrotic syndrome. Renal cyst by bacterial infection is also rare. Only one case for RVT complicated with infected renal cyst is reported in the English literature. A 78-year-old female was admitted for fever and drowsy mentality for 4 days. Contrast-enhanced computed tomography (CECT) of the abdomen showed 3.7 cm sized irregular shaped exophytic cyst well enhanced in left kidney upper pole and the left RVT. The culture of cystic fluid revealed Klebsiella pneumoniae. Our patient was effectively treated with antibiotics for 8 weeks and anticoagulant for 12 weeks. At 12-week follow-up, CECT of the kidney showed decreased cyst and nearly disappeared RVT. The possibility of RVT in patients with renal cyst infection by bacteria warrants consideration.
Keywords
Bacterial infection
renal cyst
renal vein thrombosis

Introduction
Renal vein thrombosis (RVT) is a life-threatening condition that commonly occurs with nephrotic syndrome including membranous glomerulonephritis, trauma, aortic aneurysms, oral contraceptives, and malignancies.1,2 RVT resulting from kidney infections is extremely rare.3,4 Renal cysts are commonly detected on imaging; one study reported that more than half of patients aged ≥50 years had at least one renal cyst.5 Infected renal cysts occur in approximately 2.5% of cases.6 Only one case of an infected renal cyst complicated by RVT has been reported in the literature.7
Case Report
A 78-year-old female was admitted with fever and drowsiness for the past 4 days. Her medical history included hypertension and diabetes mellitus for the past 20 years, which was well-controlled. There was no family history suggestive of thromboembolic disorders. She was on 5 mg of amlodipine, 160 mg of valsartan, 5 mg of linagliptin, and 1000 mg of metformin.
Her initial vital signs were blood pressure, 170/85 mmHg; heart rate, 95 beats/min; respiratory rate, 20 breaths/min; and temperature, 38.5°C. There were no abnormalities in her heart and lung sound. Vague left-sided costovertebral angle tenderness was noted. There was no edema or skin changes and her neurologic examination was normal.
Laboratory tests showed a white blood cell count of 9.37 × 103/mm3 with 81.8% neutrophils, hemoglobin of 9.1 g/dL, and platelet count of 264 × 103/mm3. The blood biochemistry profile was: proteins, 6.4 g/dL; albumin, 3.2 g/dL; cholesterol, 156 mg/dL; blood urea nitrogen, 17.5 mg/dL; and creatinine, 0.87 mg/dL. Her C-reactive protein (CRP) level was 78.3 mg/L and HbA1c was 7.2%. Plasma proteins C and S, and anti-thrombin III, anti-phospholipid, and anti-cardiolipin antibodies were either normal or negative. Urinalysis revealed no proteins, 1 + blood on a dipstick, 10–29 red blood cells, and 5–9 white blood cells per high-power field. Urine and blood cultures showed no bacterial growth.
Contrast-enhanced computed tomography (CECT) of the abdomen was done immediately to detect the focus of infection; a 3.7 cm irregular exophytic cyst was observed with an enhancement of the upper pole of the left kidney. The left renal vein was dilated and thrombosed [Figure 1]. Ultrasound-guided cystic aspiration was performed and approximately 7 mL of greenish pus was analyzed and cultured. The cystic fluid culture yielded Klebsiella pneumoniae, which was sensitive to ciprofloxacin.
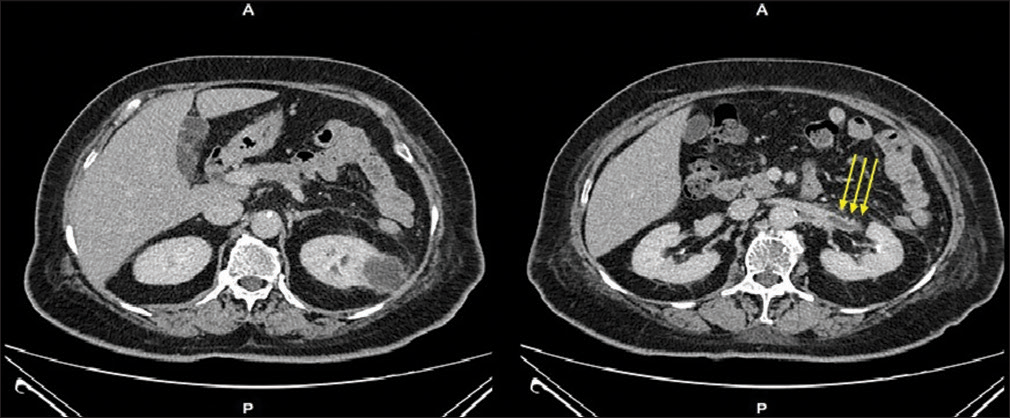
- CECT images showing a 3.7 cm sized exophytic cystic mass-like lesion with an irregular margin in the left kidney upper pole and left RVT (long yellow arrows).
The patient was treated with intravenous ciprofloxacin (400 mg/day) and apixaban (2.5 mg bid) for the initial 2 weeks. Her fever subsided on the fourth day of hospitalization, with a gradual reduction in her CRP level. Oral ciprofloxacin (250 mg bid) was subsequently administered for another 6 weeks. Apixaban was continued for 12 weeks. At the 12-week follow-up exam, CECT of the kidney showed near-complete resolution of the RVT and a decrease in the size of the renal cyst [Figure 2]. The patient remains on follow-up through our outpatient department, with no recurrence of fever and normal CRP levels after 1 year.
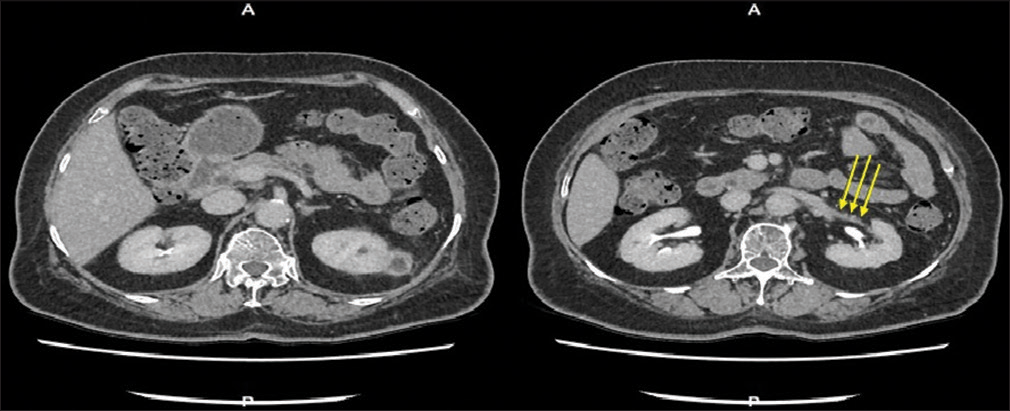
- Follow-up CT scan after 12-week treatment showing decreased size (2.3 cm) of a renal cyst with a thickened wall on the left kidney and nearly complete resolution of the left RVT (long yellow arrows).
Discussion
This case was significant because life-threatening RVT may complicate infected renal cysts. Renal cysts can become infected by direct cyst penetration during biopsies or surgical procedures, hematogenous spread of infection, and local extension from an infected collecting system or infected renal parenchyma.8,9 Initial management against cyst infection includes intravenous lipid-soluble antibiotics, such as fluoroquinolones. Cyst drainage is usually recommended in cases resistant to antibiotics, large infected cysts (>5 cm in diameter), and severe cyst infections.9 Only aspiration was performed to acquire cystic fluid for culture in our case. As a result, the infected renal cyst was treated with appropriate antibiotics for 6 weeks and cyst aspiration, without the need for further drainage or surgical intervention.
RVT may have been caused by an endotoxin-induced procoagulant state in our patient.10 Bacterial endotoxins are lipopolysaccharides found in the cell walls of Gram-negative bacteria that can induce endothelial surface changes and stimulate the expression of tissue factor, a procoagulant molecule that significantly enhances the activity of coagulation factors VIIa and Xa. Endotoxins also augment the production of the fibrinolytic inhibitor plasminogen activator inhibitor-1 by endothelial cells.10 These mechanisms may be responsible for RVT caused by infected renal cysts.
A previous study reported a case of an infected renal cyst complicated by RVT that was treated using antibiotics, cyst drainage, sclerotherapy, and thrombolytic therapy.7 In our case, the cyst was not drained because the patient responded well to conservative treatment. Oral factor Xa inhibitors have been reported in a patient with RVT, nephrotic syndrome, and pulmonary embolism.11 Our case was the first to use factor Xa inhibitors for the treatment of RVT associated with a bacterial renal infection.
Conclusion
In conclusion, physicians recognize that RVT could be complicated by an infected renal cyst, and co-administration of a factor Xa inhibitor and targeted antibiotics for a long duration is necessary for the resolution of two diseases.
Ethics approval and consent to participate
We respected all patients’ rights to privacy and protected their identities. The study protocol was approved by the Institutional Review Board of Gyeongsang National University Hospital (IRB no. 2022-11-023). All individual information was de-identified. Informed consent was obtained from the patient to write and publish her case as a case report.
Conflicts of interest
There are no conflicts of interest.
References
- Renal vein thrombosis and nephrotic syndrome: A prospective study of 36 adult patients. Ann Intern Med. 1975;83:8-14.
- [CrossRef] [PubMed] [Google Scholar]
- Renal vein thrombosis treated with thrombolytic therapy: Case report and brief review. Am J Kidney Dis. 1995;25:801-6.
- [CrossRef] [PubMed] [Google Scholar]
- Renal vein thrombosis: An underdiagnosed complication of multiple renal abnormalities. Radiology. 1979;132:43-50.
- [CrossRef] [PubMed] [Google Scholar]
- Xanthogranulomatous perinephritis: Unusual cause of renal vein and vena caval thrombosis. Urol Radiol. 1985;7:35-8.
- [CrossRef] [PubMed] [Google Scholar]
- Simple renal cysts in children: Diagnosis and follow-up with US. Radiology. 1991;178:383-5.
- [CrossRef] [PubMed] [Google Scholar]
- Infected renal cyst simulating acute abdomen. Case report. Acta Chir Scand. 1989;155:135.
- [PubMed] [Google Scholar]
- Infected renal cyst: Unusual cause of renal vein thrombosis. Eur J Rad Extra. 2005;55:97-9.
- [CrossRef] [Google Scholar]
- An infected renal cyst communicating with the urinary tract: A case report (Article in Japanese) Hinyokika Kiyo. 2014;60:485-8.
- [PubMed] [Google Scholar]
- Cyst infection in autosomal dominant polycystic kidney disease: Our experience at Toranomon Hospital and future issues. Clin Exp Nephrol. 2020;24:748-61.
- [CrossRef] [PubMed] [Google Scholar]
- Inflammation and thrombosis: The clot thickens. Criculation. 2001;103:1718-20.
- [CrossRef] [PubMed] [Google Scholar]
- Edoxaban was effective for treating renal vein thrombosis in a patient with nephritic syndrome. Intern Med. 2017;56:2307-10.
- [CrossRef] [PubMed] [Google Scholar]




