

Translate this page into:
A Very Rare Unexpected Fatal Complication of Nephrotic Syndrome
Address for correspondence: Dr. Praveen Kumar Etta, Department of Nephrology and Renal Transplantation, Virinchi Hospitals, Hyderabad, Telangana, India. E-mail: drpraveen85@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Hypercoagulability-related complications are well known in nephrotic syndrome (NS) especially in membranous nephropathy (MN). Herein, we report a case of MN complicated with acute bilateral renal vein thrombosis (RVT) with extensive involvement of inferior vena cava (IVC) and bilateral common iliac veins, with possible left renal infarction, progressing to a fatal event.
A 47-year-old man presented with anasarca of 2 weeks and left flank pain of 3-day duration. On examination, he had pitting pedal edema and high blood pressure (150/90 mm Hg). Rest of the systemic examination was unremarkable. The laboratory findings showed hemoglobin of 14.2 g/dL, serum creatinine of 1.4 mg/dL, and serum albumin of 2.2 g/dL. Urine examination showed 3+ albumin, 10–12 erythrocytes/hpf, and 5-6 white blood cells/hpf, and spot urine protein creatinine ratio was 12.3. He was diagnosed with adult onset NS.
Serology for hepatitis B and C, human immunodeficiency virus (HIV), and antinuclear antibody was negative. Serum complement levels were normal. Serum protein electrophoresis was not suggestive of monoclonal gammopathy. Urine culture was sterile. Ultrasonography showed bilateral mild bulky kidneys with prominent left renal vein with suspicion of renal vein thrombosis (RVT). He was managed by performing renal biopsy (from right kidney) followed by contrast enhanced computed tomography of abdomen, which revealed extensive inferior vena cava (IVC), bilateral RVT (left > right), and common iliac vein thrombosis; hypoperfusion of left kidney with mild perinephric fat stranding was also noted [Figure 1]. On Doppler, there was no evidence of deep vein thrombosis (DVT) in lower extremities. In view of this life-threatening vascular complication, anticoagulation was initiated after 6 h of biopsy with close monitoring along with empirical steroid therapy. He was planned for further evaluation and testing for other procoagulant conditions including antiphospholipid antibody syndrome.
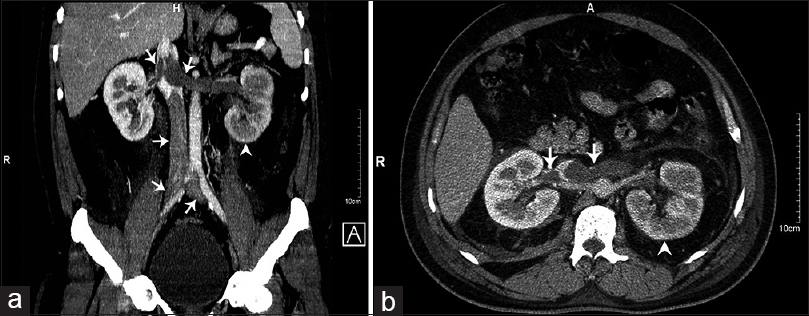
- Composite picture (panel a and b) of contrast enhanced computed tomography axial and coronal images showing extensive inferior vena cava, bilateral common iliac vein and bilateral renal vein (left > right) thrombosis (arrows pointing prominent veins with filling defects suggesting luminal thrombosis), mild bulky kidneys, hypoperfusion of left kidney (arrow heads), and mild bilateral perinephric fat stranding
Renal biopsy findings: on light microscopy, glomeruli showed mild and variable increase in mesangial matrix with a uniform and diffuse thickening of basement membrane having subepithelial spikes suggestive of MN. Immunofluorescence showed significant peripheral, fine granular deposits of immunoglobulin IgG and complement C3. Immunohistochemistry confirmed PLA2R-mediated MN. Serology for anti-PLA2R antibody test could not be done in this case.
He was advised for vascular intervention with mechanical thrombectomy and IVC filter placement. He did not consent for the same, hence conservative treatment was continued. The next day, patient had left against medical advice but succumbed immediately after leaving hospital.
NS is associated with hypercoagulability and these patients are at increased risk for DVT and RVT. Among the causes of NS, risk of thrombosis appears to be highest in patients with MN.[1] A variety of hemostatic abnormalities have been identified in patients with NS; some of these include reduced levels of antithrombin and plasminogen, increased platelet activation, and hyperfibrinogenemia. The risk is further aggravated with immobilization and hemoconcentration due to diuretic use. Severity of hypoalbuminemia is an independent risk factor; a serum albumin concentration of ≤2.8 g/dL was identified as the threshold level for increased risk in patients with MN.[2]
DVT of the extremities is the most common type of thrombotic event in these patients. RVT is an uncommon complication of NS, often clinically silent and under diagnosed because of its variable clinical and radiological findings; but with improvement in imaging techniques, it became more frequently recognizable clinical entity. RVT is more often presents as a complication of NS, though RVT itself may provoke proteinuria. It usually presents with flank pain, microscopic or gross hematuria, and enlarged kidneys with elevated serum lactate dehydrogenase (LDH) level. In severe cases, it may progress to renal infarction. Bilateral RVT can present with acute renal failure. In our case, significant renal failure has not resulted presumably due to incomplete involvement on right side; near total occlusion on left side resulted in renal infarction.
The standard therapy consists of anticoagulation with heparin followed by warfarin. These patients may have resistance to heparin therapy due to deficiency of antithrombin. The use of newer oral anticoagulants like apixaban and rivaroxaban (factor Xa inhibitors), and dabigatran (direct thrombin inhibitor) have not been studied in these patients. Bernie et al. suggested that anticoagulation alone may be sufficient for isolated left RVT because of extensive collateral venous drainage on left side, while thrombectomy may be required if the RVT is acute, bilateral, or on the right side.[3] Fein et al. reported first two successful cases of bilateral RVT with NS treated by thrombectomy.[4] Few other case reports also showed successful therapy with percutaneous thrombectomy and local thrombolysis in patients with acute RVT.[5] Surgical thrombectomy should be considered as a last resort when other therapies fail. Suprarenal IVC filters are usually preferred in patients who are at high risk for or having pulmonary embolism with DVT, or contraindication to anticoagulation.[6]
Although the reports of localized RVT or DVT as a complication of NS are well known, reports of bilateral RVT and extensive IVC thrombosis extending caudally into iliac veins in patients with NS are relatively rare. These cases had a poor prognosis. In summary, our patient with adult onset NS having MN on renal biopsy was complicated with acute extensive thrombosis involving IVC, bilateral renal, and common iliac veins, with possible left renal infarction, which seems to be a very rare phenomenon. Patient's clinical condition deteriorated due to his underlying condition and he succumbed to his illness. Our case highlights that high index of suspicion, early diagnosis and aggressive management may help to salvage these patients.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Disease-specific risk of venous thromboembolic events is increased in idiopathic glomerulonephritis. Kidney Int. 2012;81:190-5.
- [Google Scholar]
- Venous thromboembolism in patients with membranous nephropathy. Clin J Am Soc Nephrol. 2012;7:43-51.
- [Google Scholar]
- Renal vein thrombectomy for the treatment of renal vein thrombosis associated with the nephrotic syndrome. J Urol. 1968;99:1-13.
- [Google Scholar]
- Catheter-directed thrombectomy and thrombolysis for acute renal vein thrombosis. J Vasc Interv Radiol. 2006;17:815-22.
- [Google Scholar]
- Late results of suprarenal Greenfield vena cava filter placement. Arch Surg. 1992;127:969-73.
- [Google Scholar]




