

Translate this page into:
Polycythemia in hepatits C seropositive end stage renal disease patients: Role of insulin like growth factor 1
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
We present two end stage kidney disease patients who were initially erythrocyte sensitizing agent (ESA) dependent, but subsequently developed polycythemia in spite of stopping the ESA.
A 39-year-old gentleman with chronic glomerulonephritis was on maintenance haemodialysis since 2007. Serology for hepatitis C virus (HCV), hepatitis B virus (HBV) and human immunodeficiency virus (HIV) were negative. He was initially on weekly 4,000 units of erythropoietin alpha S/C. Since there was disproportionate rise in his hemoglobin with this, we stopped his erythropoietin in December 2011. But his hemoglobin continued to be in normal to high normal range (13.5-15.5 g%). Biochemical investigations are noted in Table 1. Secondary causes of polycythemia were ruled out. The yearly viral marker screening done in March 2012 showed positivity for HCV.
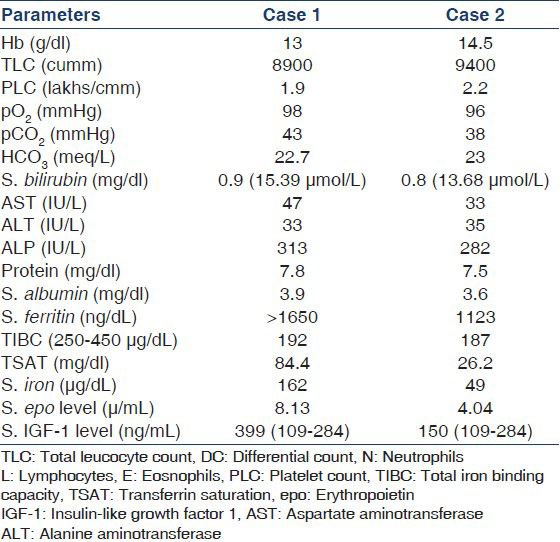
The second case, a 43-year-old man was on maintenance haemodialysis since March 2010. He was negative for HCV, HBV and HIV. He was on darbepoetin 40 μg on alternate weeks with which he maintained a haemoglobin between 10 g/dL and 11 g/dL. Since December 2011, a steady rise in haemoglobin was noticed which reached 15.5 g/dL. We stopped ESA in February 2012. Blood investigations noted in Table 1. Here again, secondary causes of polycythemia were ruled out. This patient was again detected to be positive for HCV in March 2012 during the yearly screening.
In short, we have two patients with end-stage renal disease (ESRD) having erythrocytosis in spite of stopping ESA. There were no obvious causes for secondary polycythaemia. They were subsequently detected to have HCV hepatitis on yearly screening. First patient is having features of iron overload and the second patient that of chronic inflammation, both of which can be explained by the presence of chronic hepatitis C infection.
Anaemia is invariabe in patients with chronic kidney disease except for some patients with cystic kidney disease.[1] Erythrocytosis has been observed in ESRD patients with hepatitis C.[2] HCV positivity, as in our subjects, was associated with absence of anaemia in a cohert of ESRD patients.[3] Another observation study has shown a decrease in erythropoietin requirement in ESRD patients who are HCV positive.[4] Liver can produce erythropoietin as is well known in in utero state. However, contradictory findings have been shown in different studies regarding association of elevated erythropoietin levels associated with erythrocytosis in ESRD.[2] Both our patients had low normal levels of serum erythropoietin levels. Insulin like growth factor 1 (IGF-1) plays an important role in post-transplant erythrocytosis.[5] Serum IGF-1 levels are significantly elevated in ESRD patients and erythrocytosis compared to normal subjects and ESRD patients with anaemia.[1] It has been demonstrated that IGF-1 enhanced human erythropoetic progenitor cell growth in vitro.[6] Another study has shown increased sensitivity of haemopoetic cells to IGF-1 in ESRD patients without anaemia.[7] Thus HCV positivity has shown to be associated with erythrocytosis in ESRD. We postulate that in ESRD patients with HCV infection, IGF-1 (which is produced by liver)/IGF-1 related pathway may be responsible for erythrocytosis. Our first patient had elevated serum IGF-1 and the second had normal IGF-1. In the latter patient, increased sensitivity to IGF-1 may be mediating erythrocytosis. This requires further studies.
References
- Erythropoiesis associated with viral hepatitis in end stage renal disease. Am J Med Sci. 1984;287:56-8.
- [Google Scholar]
- Factors related to the absence of anemia in hemodialysis patients. Blood Purif. 2011;32:69-74.
- [Google Scholar]
- Effect of hepatitis C infection on anemia in hemodialysis patients. Hemodial Int. 2008;12:94-9.
- [Google Scholar]
- Effects of losartan or enalapril on hemoglobin, circulating erythropoietin, and insulin-like growth factor-1 in patients with and without posttransplant erythrocytosis. Am J Kidney Dis. 2002;39:600-8.
- [Google Scholar]
- Insulin-like growth factor I plays a role in regulating erythropoiesis in patients with end-stage renal disease and erythrocytosis. J Am Soc Nephrol. 1999;10:315-22.
- [Google Scholar]




