

Translate this page into:
Cystic partially differentiated nephroblastoma: A rare renal tumor
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 2-year-old female child presented with gradually increasing painless mass on the left side of the abdomen since 2 months. No history of fever, hematuria, weight loss, anorexia or burning micturation was present. Physical examination revealed large, hard and non-tender left sided abdominal mass, which was ballotable on palpation. Blood biochemistry, urinalysis, renal and liver function tests were within the normal limits.
Ultrasonography revealed large well-circumscribed, multi-cystic abdomino-pelvic mass lesion arising from the left kidney. This multi-cystic mass showed variable sized anechoic cysts with intervening septa with no echogenic debris [Figure 1]. No communication between the cysts was seen. Rests of the abdominal organs were normal. Contrast-enhanced computed tomography was done for further characterization, which showed large 16 cm × 11 cm multi-cystic abdomino-pelvic mass arising from the left kidney and occupying whole of left abdomen [Figure 2]. Patient underwent open nephrectomy. Intra-operatively, multi-cystic lesion contained within the capsule arising from left kidney was seen [Figure 3]. Histopathological examination revealed immature blastemal elements in the septa and a diagnosis of cystic partially differentiated nephroblastoma (CPDN) was made.
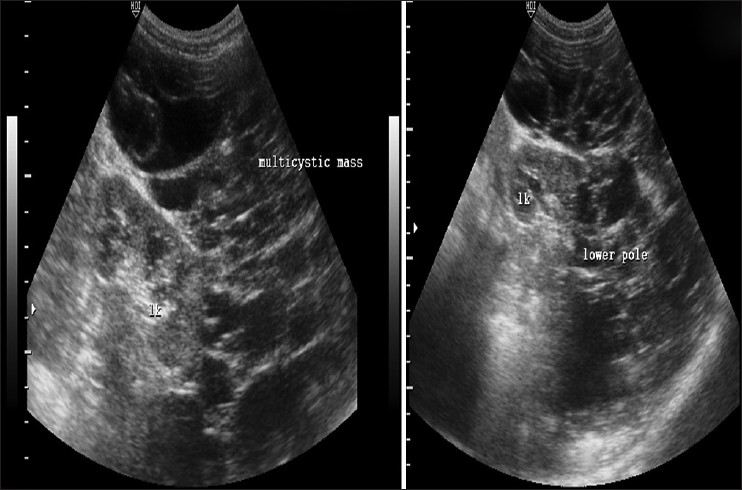
- Ultrasonography showing a large multi-cystic lesion arising from the lower pole of the left kidney. No communication with pelvicalyceal system is seen

- (a) Computed tomography (CT) scannogram showing abdominal distension with homogenous haze (arrows) predominantly on the left side of the abdomen with mild displacement of the bowel loops to the right (b) Coronal reconstructed CT images showing multicystic mass arising from the left kidney (arrow) extending from the left hypochondrium to the pelvis, crossing the midline and reaching to the right side of the abdomen with displacement of bowel loops on the right side

- Intra-operative images showing well-circumscribed multi cystic lesion contained within a capsul
CPDN is a variant of multilocular cystic renal tumor (MCRT). Other variant of MCRT is cystic nephroma (CN).[1] MCRT presents as an abdominal mass and most children present in the first 2 years of life, with a male predominance. Biphasic age distribution is more common in girls: 4-20 years of age and fifth to sixth decades. CPDN and CN are indistinguishable on gross examination. On imaging alone, CPDN cannot be differentiated from CN in this age group. Histopathology shows blastemal cells within the septa, which clinches the diagnosis of CPDN.[1] According to Joshi and Beckwith[23] diagnostic criteria for CPDN includes well-defined multicystic mass, presence of thin septa, absence of solid enhancing nodules and histological evidence of cysts lined by flattened cuboidal epithelium with septa containing blastema, embryonal stroma or epithelium element. Management of CPDN is nephrectomy alone.
All cases of CN follow a benign course. However, CPDN may show aggressive behavior and has a tendency for recurrence following surgery due to the presence of blastemal cells in septa, despite the usual benign course of the tumor.
The main differential diagnoses are cystic Wilm's tumor, cystic variants of mesoblastic nephroma, segmental multicystic dysplastic kidney, localized cystic kidney disease, polycystic kidneys and renal hydatid. Identification of solid nodular components should suggest the diagnosis of Wilm's tumor. Mesoblastic nephroma is congenital and shows solid component within. Antenatal ultrasound shows tumor usually arising from the lower pole of the kidney. Polycystic kidneys are bilateral, involve the kidneys diffusely and associated with cysts in other organs. Multicystic dysplastic kidneys do not show excretion of contrast. Hydatid cysts show the presence of daughter cysts within the mother cyst.
Acknowledgment
We would like to thank Dr. Pragya Singh for her contributions.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Multilocular cyst of the kidney (cystic nephroma) and cystic, partially differentiated nephroblastoma. Terminology and criteria for diagnosis. Cancer. 1989;64:466-79.
- [Google Scholar]
- Pathologic delineation of the papillonodular type of cystic partially differentiated nephroblastoma. A review of 11 cases. Cancer. 1990;66:1568-77.
- [Google Scholar]




