

Translate this page into:
Recurrent lactic acidosis secondary to hand sanitizer ingestion
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Due to their ability to decrease the spread of infection, hand sanitizers are now ubiquitous in health care settings. We present the case of a 50-year-old woman who was admitted with acute alcohol intoxication and had near complete recovery in 12 hrs. Subsequently, she was found unresponsive on the floor of her hospital room on two separate occasions. Evaluations revealed repeatedly elevated levels of ethanol, acetone, and lactate as well as increased anion gap and hypotension, requiring intensive care unit evaluation and intubation for airway protection. During the second episode, she was found next to an empty bottle of ethanol-based hospital hand sanitizer. She confirmed ingesting hand sanitizer in order to become intoxicated.
Keywords
Acidosis
alcohol
anion gap
hand sanitizers

Introduction
Hand sanitizers are either ethanol or isopropanol based, but may contain a mixture of isopropanol (isopropyl alcohol), 1-propanol, 2-propanol, and acetone. Hand sanitizers contain 60-95% alcohol by volume.[12] In comparison, vodka contains 40% alcohol and beer contains 4-6% alcohol. Because of the high alcohol content that is rapidly absorbed, hand sanitizers are becoming an attractive form of both toxic ingestion and suicide attempts.[3] Accidental ingestion by children has led to cases of morbidity.[4] Unrestricted public access has allowed for the increasing popularity among teenagers and adults. We encountered a patient who repeatedly became intoxicated on hand sanitizers during her hospital stay, which is unique in its nature both from diagnosis and management prospective.
Case Report
A 50-year-old woman was admitted for altered mental status in the setting of acute alcohol intoxication. She admitted to binge drinking an unknown quantity of wine 12 hrs prior to admission. On arrival, her vital signs were normal except for a blood pressure of 88/58 mm Hg. She was drowsy, but arousable and partially oriented. Laboratory evaluation showed a blood alcohol level of 353 mg/dl, anion gap of 17, lactate of 4.5 mmol/L (normal 0.6-2.3 mmol/L), beta hydroxybutyrate of 0.7 mmol/L (normal <0.4 mmol/L), positive urine ketones, and serum glucose of 80 mg/dl. The patient had a serum osmolality of 383 mOsm/kg; a normal serum osmolal gap when adjusted for the elevated ethanol and undetectable levels of methanol, isopropanol, and acetone. She received 7 L of normal saline for hypotension. Twelve hours after admission, her serum alcohol, anion gap, lactate, serum ketones, hypotension, and mental status had normalized. Workup for sepsis was unremarkable.
One day later, she was found unresponsive on the floor of her hospital room with a blood pressure of 93/60 mm of Hg and a Glasgow Coma Score of 3. She required fluid resuscitation and intubation for airway protection. Computed tomography (CT) of the head was unremarkable. Her lactate and anion gap had increased to 4.5 mmol/L and 17, respectively. One day later, she was extubated and her serum lactate and anion gaps had normalized to 1.4 mmol/L and 7, respectively. Her mental status returned to alert and fully oriented.
Two days later, the patient was again found in her hospital room unresponsive, this time next to an open and an empty bottle of ethanol based hospital hand sanitizer. Her vital signs were normal and her Glasgow Coma Score was 3. Repeat head CT was unremarkable. Laboratory evaluation showed a lactate of 3.9 mmol/L, anion gap of 15, serum ethanol of 362 mg/dl, methanol of 0 mg/dl, acetone of 11 mg/dl, and isopropanol of 14 mg/dl. Arterial blood gas showed a pH of 7.32, PaCO243 mm Hg, PaO273 mm Hg, and bicarbonate 22 mmol/L. She was admitted to the intensive care unit for altered mental status, where she required nasopharyngeal airway and supportive care. Over the next 6 hour, her mental status, elevated lactate levels, and metabolic acidosis gradually returned to normal. The patient admitted to drinking ethanol based hospital hand sanitizer with a goal to become intoxicated. She denied suicidality. Hand sanitizers were removed from her room and she was placed on one-to-one monitoring. She was discharged without further incident to an in-patient alcohol treatment program.
Discussion
Hand sanitizers are either ethanol- or isopropanol- (isopropyl alcohol) based and contain about 50-100% more alcohol than vodka. To reduce the spread of infection, the United States Centers for Disease Control and many hospital guidelines recommend hand sanitizer use before and after every patient encounter.[5] Thus, sanitizer bottles have become ubiquitous inside and outside of patient rooms.
Our patient exhibited most of the classic symptoms of acute ethanol intoxication including central nervous system depression, respiratory depression, lactic acidosis, ketoacidosis, and nausea. Ethanol can cause peripheral vasodilation and hypovolemia, which is the likely etiology of the profound hypotension seen in our patient. Other possible symptoms of ethanol intoxication include cardiac arrhythmia, acute liver injury, myoglobinuria, hypokalemia, hypomagnesemia, hypocalcemia, and hypophosphatemia. Risk of respiratory depression and arrest increases with serum ethanol levels ≥300 mg/dl. Cardiac arrest and death usually occurs with ethanol levels ≥500 mg/dl, although death has been reported at lower levels and there are case reports of patients with high tolerance surviving with levels ≥1200 mg/dl.[6]
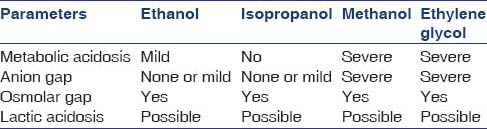
Isopropanol-based sanitizer intoxication presents with symptoms similar to ethanol toxicity including central nervous system and respiratory depression. Large ingestions can also lead to profound hypotension. Death has been noted with plasma concentrations levels ≥400 mg/dl.[7] A fruity odor suggestive of ketosis is often present. Classic laboratory findings include an elevated osmolal gap and ketonemia with no evidence for an anion gap metabolic acidosis [Table 1]. Aside from hand sanitizers, isopropanol is also found in numerous household cleaners and is the primary ingredient of rubbing alcohol.[67]
In a patient with compatible symptoms, a diagnosis of hand sanitizer ingestion is confirmed with visual witness of ingestion by hospital staff or patient admission to ingestion when questioned. Even without confirming evidence, ingestion should be suspected with recurrent intoxications in the hospital. Recurrent or worsening clinical status should prompt laboratory evaluations for toxic ingestion.
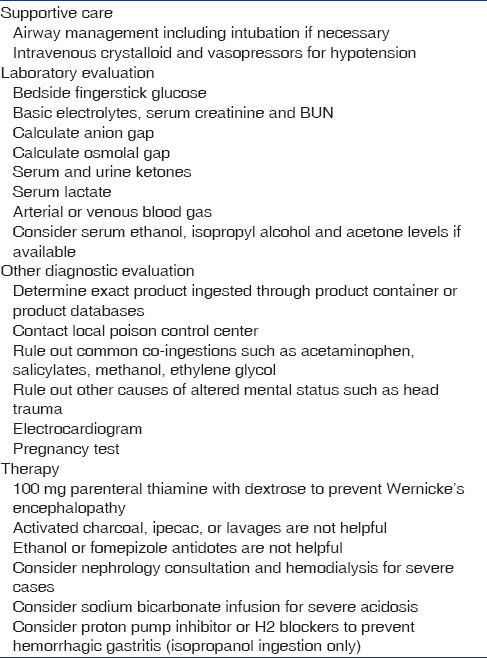
Treatment of both ethanol and isopropanol intoxication is largely supportive, including airway and respiratory support [Table 2]. Aggressive fluid resuscitation and vasopressors may be necessary for hypotension. Metabolic derangements must be corrected, especially hypoglycemia, which may be life-threatening. Both ethanol and isopropanol are rapidly and completely absorbed after oral ingestion. Therefore, there is little clinical utility for activated charcoal or gastric lavage for suspected ingestions. Hemodialysis effectively removes isopropanol and its metabolite acetone as well as ethanol and is indicated for life-threatening ingestions with elevated serum ethanol or isopropanol levels ≥400 mg/dl, coma, respiratory failure requiring intubation, or hypotension requiring pressors. Patients with underlying hepatic dysfunction may be more likely to require hemodialysis. All patients should receive thiamine to prevent or treat underlying Wernicke's encephalopathy.[68]
While inhibition of alcohol dehydrogenase with the administration of fomepizole or ethanol is indicated with suspected methanol or ethylene glycol ingestions, it is contraindicated for use with suspected ethanol or isopropanol-based hand sanitizer ingestions. Alcohol dehydrogenase inhibition prevents isopropanol metabolism to its less toxic metabolite, acetone, and prolongs the half-life of ethanol. Therefore, administration of fomepizole or ethanol may prolong the toxic effects of ethanol and isopropanol and gives no added clinical benefit. Novel therapies such as metadoxine, a pyrrolidone carboxylate of pyridoxine, are currently under investigation. Metadoxine has been shown to result in a more rapid ethanol clearance compared with placebo, but is not yet approved for use in the United States.[9]
Conclusion
Recurrent hand sanitizer ingestion is common, even when a diagnosis of hand sanitizer ingestion has been made and discussed with the patient. Efforts to prevent initial or recurrent ingestion should be pursued for high-risk individuals. Proposed solutions based on observational data include routine removal of hand sanitizers from patient rooms, one-on-one monitoring, building tamper proof containers, and utilizing foam versus gel preparations.[10] Our institutional order sets for suspected alcohol ingestion now contain automatic orders to remove hand sanitizers. Locked, self-contained, wall-based pumps, which only deliver one squirt of sanitizer, may prevent large dose ingestion compared to free standing bottles whose lids can be readily unscrewed,[11] as was the case in our patient. Hospitals should undergo systematic quality improvement aimed to prevent in-hospital intoxications while maintaining adequate hand hygiene.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Ingestion of hand sanitizer by a hospitalized patient with a history of alcohol abuse. Am J Health Syst Pharm. 2008;65:2203-4.
- [Google Scholar]
- Intoxication of a prison inmate with an ethyl alcohol-based hand sanitizer. N Engl J Med. 2007;356:529-30.
- [Google Scholar]
- The rising incidence of intentional ingestion of ethanol-containing hand sanitizers. Crit Care Med. 2012;40:290-4.
- [Google Scholar]
- Acute ethanol poisoning in a 4-year-old as a result of ethanol-based hand-sanitizer ingestion. Pediatr Emerg Care. 2010;26:508-9.
- [Google Scholar]
- Healthcare Infection Control Practices Advisory Committee; HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. MMWR Recomm Rep. 2002;51:1-45.
- [Google Scholar]
- Isopropyl alcohol intoxication: A diagnostic challenge. Am J Kidney Dis. 2002;40:E12.
- [Google Scholar]
- Treatment of the alcohol intoxications: Ethylene glycol, methanol and isopropanol. Curr Opin Nephrol Hypertens. 2000;9:695-701.
- [Google Scholar]
- Metadoxine in acute alcohol intoxication: A double-blind, randomized, placebo-controlled study. Alcohol Clin Exp Res. 2002;26:340-6.
- [Google Scholar]
- Changing dispensers may prevent intoxication from isopropanol and ethyl alcohol-based hand sanitizers. Ann Emerg Med. 2007;50:486.
- [Google Scholar]




