

Translate this page into:
Renal tuberculosis with lobar calcification
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 32-year-old male presented with right-sided abdominal pain. Physical examination revealed right-sided renal angle tenderness. The temperature was 38.7°C and blood pressure 170/82 mmHg. The hemogram and biochemistries were within the normal limits except for elevated serum creatinine levels (1.8 mg/dl). X-ray of the abdomen and pelvis showed small right kidney with pathognomonic lobar calcification, with calcific rims around the distorted lobes, along with ureteric calcification [Figure 1a]. Computerized tomography (CT) confirmed the findings of lobar renal calcifications with ureteric calcification suggesting genito-urinary tuberculosis (TB) [Figure 1b]. There was history of pulmonary TB at the age of 19, for which he had taken anti-tuberculous treatment for 6 months. The diagnosis of urinary TB was confirmed by urine culture. The patient was started on anti-tuberculous treatment and surgery was advised for the management of hypertension but the patient refused.
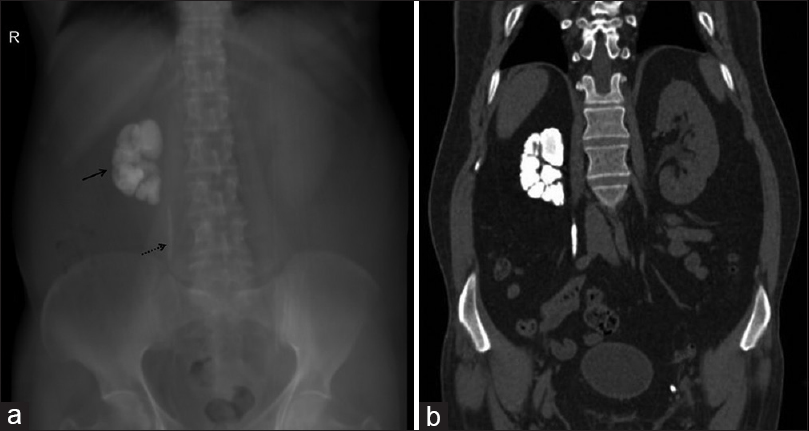
- (a) Antero-posterior view of X-ray of abdomen and pelvis showing shrunken right kidney with pathognomic lobar calcification, with calcific rims around the distorted renal lobes. There is associated linear calcification in right lower paravertebral region suggesting ureteric calcification. (b) Coronal section of computerized tomography of abdomen and pelvis showing shrunken right kidney with lobar calcification and right ureteric calcification suggesting genito-urinary tuberculosis with extra-renal spread of infection
Tuberculosis of the genito-urinary tract usually affects adults between 20 and 40 years of age and is rare in children.[1] Diagnosis is usually delayed because of insidious onset and nonspecific symptoms of presentation such as fever, weight loss, anorexia, abdominal pain, dysuria and sometimes hematuria.[1]
The causative organism is usually Mycobacterium tuberculosis, which disseminates hematogenously or lymphatically to the kidneys.[12]
The pattern of presentation of calcification ranges from initial faint and punctate to later coalescing. Focal granulomatous mass is usually encountered with focal lobar calcifications. The occurrence of ureteral calcification along with renal calcifications further proves the diagnosis of lobar presentation and generally has unfavorable prognosis.[13]
Intravenous urogram is regarded as the investigations of choice that provides with anatomical and functional details. Earliest findings include minimal calyceal dilatation with the loss of calyceal sharpness. Ultrasonography or CT plays an important role not only in evaluating nonfunctioning kidneys but also in patients with complications of renal TB such as perinephritis, perinephric abscess, fistulae, psoas abscesses and rarely renal failure.[14]
Source of Support: Nil
Conflict of Interest: None declared.
References
- Tuberculosis of the genitourinary system-Urinary tract tuberculosis: Renal tuberculosis-Part I. Indian J Radiol Imaging. 2013;23:46-63.
- [Google Scholar]
- Mycobacterial infection after renal transplantation - Report of 14 cases and review of the literature. Q J Med. 1990;77:1039-60.
- [Google Scholar]
- Roentgenographic findings in urinary tract tuberculosis. A 10 year review. Am J Roentgenol Radium Ther Nucl Med. 1974;121:487-99.
- [Google Scholar]
- Clinical presentation and diagnostic approach in cases of genitourinary tuberculosis. Indian J Urol. 2008;24:401-5.
- [Google Scholar]




