

Translate this page into:
Diabetes, hypertension, sanitation, and health education by high school students in Guyana, South America
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
We initiated a program for early detection of diabetes and hypertension, the main causes of kidney failure in Guyana, South America. We trained local high school students with the goal that these students would stay in the villages for long-term, become health advocates and shift the reliance away from physicians. This project involved 7 high school students who were taught to monitor the health of one village of 1000–1500 population each. The program will be implemented for 3 years in which the entire population of seven villages (approximately 10,000 people) will be covered. This represents 1.3% population in Guyana. We present data from the pilot study from the sample of 619 people. The prevalence of diabetes mellitus was 13.9%. Among diabetics, 33.7% were using insulin and 86% oral hypoglycemic agents. Prevalence of hypertension was 29.4%, 63.2% were overweight and 17% were obese. About 9.9% patients were unaware about the existence of hypertension. We have shown in our study that high school students can be used to collect health data and monitor diabetes and hypertension. There was also a significant incidence of undetected diabetes and hypertension.
Keywords
Diabetes
Guyana
hypertension
rural village

Introduction
The advent of the internet and global travel has increased the expectations of the people in developing countries. Renal replacement therapy (RRT) is currently nonexistent in most of the developing countries and is tantamount to a death sentence. There are some nongovernmental agencies that are providing much needed primary care to developing countries; however, a few are engaged in highly specialized surgical and medical care. Since its commencement in 2008, our humanitarian program has carried out 26 kidney transplants and numerous peritoneal dialysis catheter placements, and vascular access procedures for hemodialysis. We have also delivered lectures and held press conferences to make local doctors and patients aware of the program.[123] We visit Guyana 3–4 times a year with each visit lasting 5–7 days (21 missions so far).
After the successful launch of a program of RRT, we introduced a program of prevention and early detection of diabetes and hypertension, the main causes of kidney failure in Guyana. This project, called the SEVAK Project (www.sevakproject.org), empowers the local person living in the village to look after the health care of the people in their village. The acronym SEVAK stands for “sanitation and health education in village communities through improved awareness and knowledge of prevention/management of diseases and health promotion.” This project is modeled on the independent duty Corpsman (IDC) in the US Navy who are high school graduates interested in health care. They are given 12 months of training and then assigned to Marine Corps Units or Navy Ships.[4] They provide primary care, look at injuries, manage disasters, and also check on the preventive care of sailors along with conducting environmental checks such as humidity, temperature, and sanitation.
The SEVAK program comprised of training high school students in clinical skills such as the monitoring/recording of blood pressure (BP), blood sugar, lifestyle modification education, noting dietary practices, so that they could keep better surveillance on the health of their respective villages. This program currently encompasses 7 villages of approximately 1000–1500 people each.[56] The stipulation is that each student resides in the village and, therefore, is familiar with the environment and his/her neighbors.
Materials and Methods
SEVAK curriculum
The curriculum was developed from three prior intervention programs in India. It is evidence-based and consisted of a set of powerpoints and reading material, which includes basic anatomy, physiology, pathology, and disease processes. The 3-month course concluded by a written and oral test followed by skills testing of mock interviews, use of internet, entry of data in Excel Spreadsheet, and finally measurement of BP, and blood sugar. Rigorous attempts were made during the training to ensure minimal within and between rater variability for all SEVAKs. At the end of their training, the measurements by SEVAKs were in agreement with that of physicians.
Powerpoints and handbook
These comprise of: (1) Introduction and basic terminology. (2) The concept of SEVAKs. (3) Hypertension. (4) Diabetes. (5) Cardiovascular system including basic life support. (6) Musculoskeletal system. (7) Pulmonary system. (8) Gastroenterology. (9) Endocrinology. (10) Infectious diseases. (11) Trauma including transportation of patients and liaison with EMS. (12) Pediatrics. (13) Obstetrics: pregnancy and gestational age, hypertension, eclampsia, diabetes, and referral. (14) Gynecology: Bleeding and referral. (15) Nutrition Concepts: requirements, carbohydrate, fats, protein, and calories. (16) Exercise: importance and various concepts. (17) Lifestyle modification education. (18) Immunization: adult and child schedules and importance in prevention. (19) Preventive strategies: breast, cervix, prostate, lung, mouth and stomach cancers. (20) Preventive strategies: diabetes, hypertension, CVD and other infectious diseases. (21) Water purification. (22) Sanitation including mosquito bite prevention, toilets, etc., (23) Telemedicine-including the use of laptops. (24) Coordination of care and liaison with different levels of caregivers. (25) Data collection and analysis. (26) Lifestyle modification education.
Field work
The students have screened 619 people in the pilot phase. The entire program is to screen 200 people a month until the entire population of seven villages comprising 10,000 people are screened. Each SEVAK works over the weekend outside school hours and monitors and follows the screened families and serves as their health advocate.
Selection of villages and SEVAKS
We have selected seven villages in the remote region of Guyana where there are no medical facilities, and they are far from any health center. Each SEVAK resides in the village and is familiar with the people they are screening. In this way, the SEVAKS and the families build trust in each other for the long-term.
Monitoring of results
Pre- and post-evaluation of the training is done by the authors via internet and visits to Guyana. Our team visits Guyana every 3 months to perform kidney transplants and associated clinics.[1] During these visits, we accompany the SEVAKS in the field and monitor their progress. Particular attention is paid to visit the patients who have been diagnosed with hypertension and diabetes. We also reinforce the skills of BP and blood sugar measurement. We also ensure that measurements by SEVAKs are in agreement with that of physicians on each visit.
Statistical analysis
Chi-square test was used to assess statistical significance of the difference between categorical variables. T-test, Wilcoxon signed-rank test, analysis of variance (ANOVA), and Kruksal–Wallis ANOVA test were used for continuous variable depending upon distribution (normal or nonnormal) and number of comparison groups.[78] “R” was used for all analysis. R is open source statistical analysis software widely used for data analysis.[9]
Results
Population screening
In the pilot phase, we have screened 619 people. The results generated from the sample of 619 people can estimate the health indices in overall population of Guyana with the error rate of 3.94% and confidence level of 95%.[78] The plan is to screen 200 people a month until the entire populations of seven villages comprising 10,000 people are screened in 3 years.
Results from pilot study
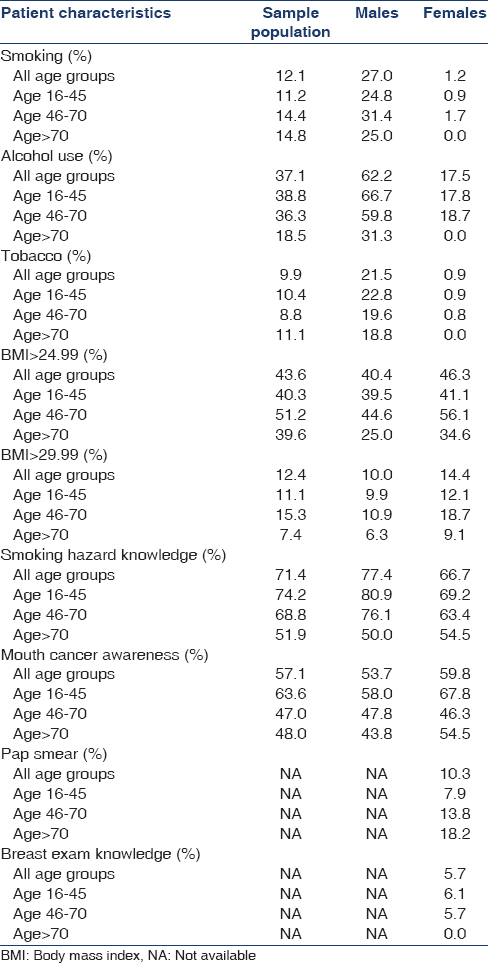
The mean age of the sample population was 42.2 years; 43.6% of them were males, 75.1% were married, 3.1% were singles, and 5.3% were widowed. The prevalence of obesity (body mass index [BMI] >29.99) was 12.4% whereas 43.6% people were overweight (BMI > 24.99). The prevalence of smoking was 12.1% and of alcohol consumption was 37%. Drug abuse was low at 0.5%. All people (100%) had access to toilet, of which 83.6% were in house and rest were out of house. The purified water (by reverse osmosis) was available to 59.3% population, whereas 35.4% used well water for drinking [Table 1].

The overall rate of pap smear testing was 10.3% in women. However, in age group of 16–45 years, rate of pap smear testing was only 7.9%. Only 5.7% women had knowledge about breast examination [Table 2].
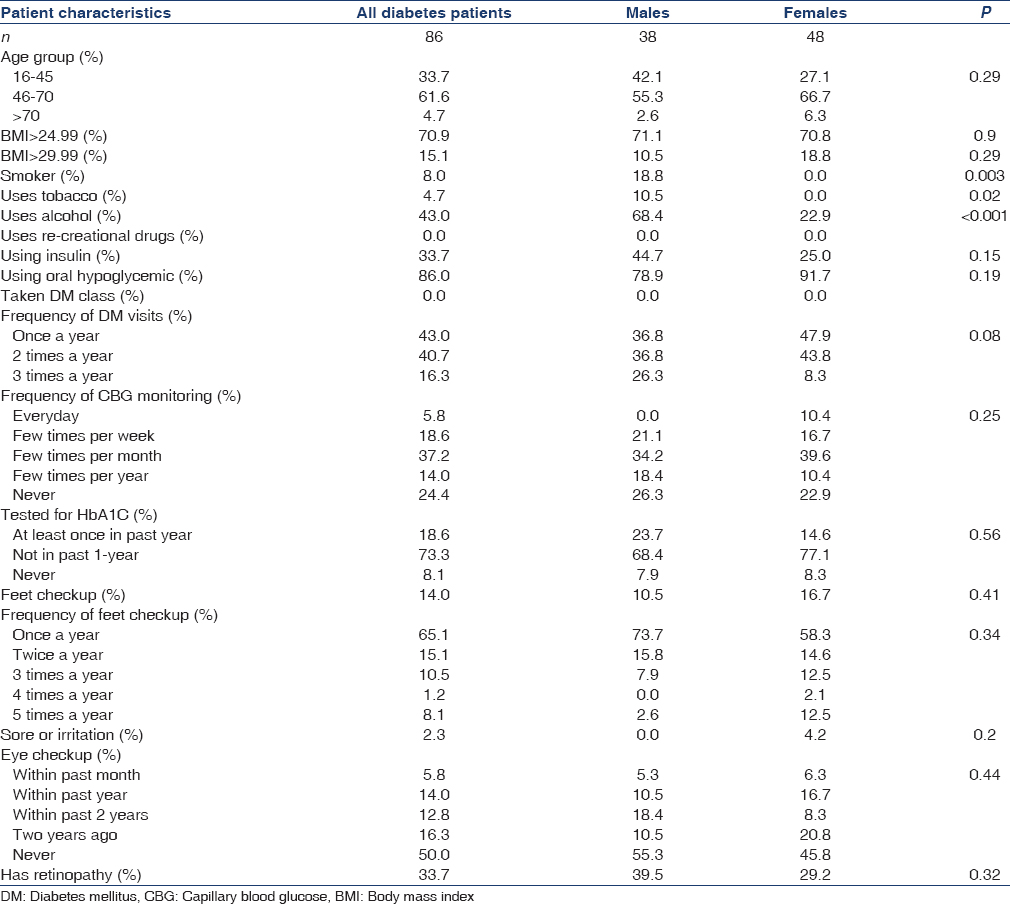
The prevalence of diabetes mellitus was 13.9%. Among diabetics, 33.7% were using insulin and 86% oral hypoglycemic. About 14.1% of diabetics had at feet checkup checked in last 1-year. About 33.7% of diabetics had retinopathy. Only 5·8% of diabetics had dilated eye exam in last 1-year [Table 3].
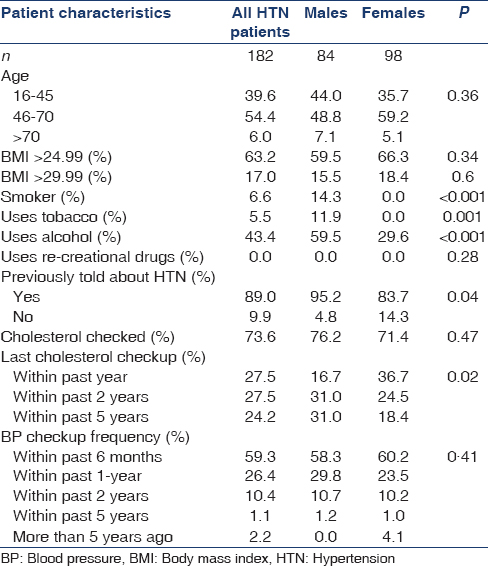
The prevalence of hypertension in Guyana was 29.4%. About 63.2% of them were overweight, and 17% were obese. Among hypertensive patients, the prevalence of smoking was 6.6%, tobacco use was 5.5%, and alcohol use was 43.4%. About 9.9% patients were unaware about the existence of hypertension [Table 4].
Discussion
The SEVAK project in Guyana was initially trialed in Gujarat, India.[5] Balagopal et al.[6] have carried out a prototype program to address the shortfalls in the healthcare needs of the villages. One village per district (n = 27) in Gujarat, India, has been chosen to screen the residents for diabetes, hypertension, obesity, and monitor those with chronic diseases. The project involves coordinating with the villages and identifying bright individuals with, medical and or nonmedical, backgrounds who are interested in the project (one per a village of 1000–1500 population), and then train to be SEVAKs. They have shown that such a program has become self-sustaining as the SEVAKs who live in the village will be able to continue the screening, delivery of care, and health education. The major difference between the Indian and Guyanese model is that the SEVAKS in Guyana are still in high school and they work in their villages only during the weekends.
The SEVAKs are also trained in good sanitation practices, safe drinking water, smoking cessation, and malaria prevention. SEVAKs maintain a database on the medical problems of the villagers and target the high-risk groups for detailed health education and monitoring. They also act as liaison between the patient and his/her physician. They will help to ensure that patients on TB, HIV, and malaria treatment are adherent with their medicines and that patients with diabetes and hypertension come for regular checkups and attend health classes. Pregnant women will be screened for diabetes, and they will be encouraged to deliver in a hospital or safe environment to decrease maternal mortality.
Vast populations in developing countries do not have access to basic health care. Numerous efforts by government and NGOs have failed to remove this disparity.[1011] It was observed in a recent study that in rural India, noncommunicable, and chronic diseases are the leading causes of death.[12] It was also observed that this pattern of death is unlikely to be unique to these villages and provided a new insight into the rapid progression of the epidemiological transition in rural India. Access to care is marginalized, and there were no primary health care centers that could manage chronic diseases.[1314] This lacuna made them even more vulnerable to chronic diseases and their complications. Seventy percent of Indian Population live in the villages[15] (700 million people). Like India and many other developing countries, Guyana is also undergoing an epidemiological transition with both noncommunicable and chronic diseases are the leading causes of death.
We have studied diabetes and hypertension in detail in the sample population of Guyana. In developing countries, burden of diabetic complications is very high compared to developed countries.[16] In Sub-Saharan Africa, up to 50% patients with type 2 diabetes have cardiomyopathy.[17] Similarly in Latin America, the prevalence of microvascular complication was estimated to be 62.8%.[18] The reason can be the lack of awareness, infrequent hospital visits, lack of routine blood glucose measurement and insufficient eye and feet examinations. We tried to assess all these factors in our study population in Guyana. Also, additive risk factors such as smoking, tobacco use, and hypertension complicate the pathophysiology of diabetes. In the sample population, 8% of the diabetics were smokers, 4.7% used tobacco, and 43% used alcohol. These characteristics were predominantly seen in males for Guyanese population.
Prior studies have shown that the prevalence of un-diagnosed hypertension is high in developing countries.[19] A recent systematic review showed that in Sub-Saharan Africa only 27% of patients were aware of their hypertension.[19] Our data showed that almost 10% of the hypertensive patients were previously undiagnosed. Follow-up measurements are very important in hypertensive patients. As SEVAKs are from the community itself and as they go themselves to the patient's home, follow-up of the patients become very efficient. Like Guyana, many of the developing countries have a significant percentage of undiagnosed hypertensive population, shortage of health care facility being the prime reason for it.[20] In such a scenario, projects like SEVAK act as a prudent alternative. In other results, 55% of the hypertensive patients had their cholesterol checked up in the past 2 years. About 6.6% of all the hypertensive patients were smokers.
The importance of educating and delivery of healthcare to this large base of developing countries in their resource-poor settings becomes an urgent issue. Large-scale efforts to improve general awareness about diabetes, hypertension, cardiovascular disease, its risk factors, and to promote healthy lifestyles are needed to reduce mortality, morbidity and improve the quality of life. SEVAK project is one such effort to meet the health care need of the rural population in Guyana. The prime feature of the project is that local community members are trained for primary screening of the diseases, so that remote areas of the country, which are underserved as such, can be benefitted by their own community members.
However, our project has limitations as SEVAKs are high school students; therefore, they need to manage their field work along with their academic study. For example, at the time of school examinations, SEVAKs may not be able to perform their duty efficiently. Also, as they are students, maintenance of their personal motivation is also a challenging task. The government of Guyana, according to a Government Information Agency release, launched the community health workers (CHW) training program in 2011 as the first step of medical training in Guyana.[21] The CHWs would be receiving specific skills and knowledge that would enable them to drive the delivery of care in the remote primary health care system. However, we could not find evidence that this program has continued, and there are no published outcomes of this effort.
To raise awareness for better health practices, the Government of India installed “Accredited Social Health Activists”, called ASHA workers, beginning in 2005. In Hindi language, the word ASHA means hope. The Health Care Program of the Government of India targeted the installation of one ASHA in every village of India, by the year 2012. As many as, 25,000 ASHA workers per state were planned. ASHA workers are usually females living in the village they work in. Equipped with familiarity of village environment and personal relationships with the other women of the village, these workers educate pregnant women of the village in healthy prenatal and postnatal practices. Instead of home-based child deliveries by inept and ill-equipped midwives, ASHA workers take the pregnant mothers to an approved hospital for deliveries in modern medical facilities under the professional care of physicians and nurses. They are paid Rs. 600 or $12 for each case, and the mother is paid Rs. 1400 or $28. For immunization of each child, the mother is paid Rs. 150 or $3. The monetary payments to ASHA workers for the various responsibilities and tasks fall below the usual standards set for health care workers in the medical profession. There have been public demonstrations by ASHA workers with slogans and banners demanding higher payments for their work. However, there are two sides of every story, and there are numerous instances in which ASHA workers have had a positive impact.[2223]
We empowered SEVAKs in Guyana to become health care advocates in their villages. Eventually, we hope to shift the reliance from physicians to motivated students who are likely to stay in their villages for the long-term. Preliminary results and feedback on the SEVAK Project from various stakeholders in both the countries have been encouraging. Future plans for the SEVAK project are to (i) produce a detailed policy paper about the lifestyle, environment, family history and BP and diabetes for the Governments of India and Guyana to inform decision making process and allocation of health care funds and (ii) continuously improve the training program based on the experience so far and extend the SEVAK to other regions of India and Guyana.
Conclusion
We have shown in our pilot study in Guyana that high school students who reside in the village can be taught the basics of survey techniques and measurement of BP and blood sugar. The seven villages selected in this pilot program are in the remote region of Guyana where there are no medical facilities, and they are far from any health center. Each SEVAK resides in the village and is familiar with the people they are screening.
To conclude, the IDC concept of the US Navy that has been tried and tested for many decades, has been modeled and modified to develop the SEVAK program in India and Guyana, South America. The broad capabilities taught through this model can produce a very capable type of community health worker that can integrate well into the country's health system. While this pilot shows the feasibility of using SEVAKs for surveillance, scalability needs to be proved by doing a large study. Feedback from various stakeholders has been positive.
Acknowledgments
Mr. George Subraj, Philanthropist and President of Zara Realty, Queens, New York, (www.zararealty.com) who supported the program and the Principal of SVN School (https://www.facebook.com/SVNGuyana), who has supported the SEVAKS.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Report of the first peritoneal dialysis program in Guyana, South America. Perit Dial Int. 2013;33:116-23.
- [Google Scholar]
- The Story of First Kidney Transplant in Guyana, South America, and Lessons Learnt for Other Developing Countries. Indiana, iUniverse 2009
- [Google Scholar]
- Hospital Corpsman – Wikipedia, The Free Encyclopedia. Available from: http://www.en.wikipedia.org/wiki/Hospital_corpsman
- Sevak Project: Improving Access to Care in Rural India. Available from: http://www.sevakproject.org/index.html
- A community-based participatory diabetes prevention and management intervention in rural India using community health workers. Diabetes Educ. 2012;38:822-34.
- [Google Scholar]
- Bureau of Statistics: A Government of Guyana Agency. Available from: http://www.statisticsguyana.gov.gy/
- Sample size determination. Influencing factors and calculation strategies for survey research. Saudi Med J. 2003;24:323-30.
- [Google Scholar]
- R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2013.
- Articles about Rural Areas – Times of India – Economic Times. Available from: http://www.articles.economictimes.indiatimes.com/keyword/rural-areas
- Burden of Disease in India. Available from: http://www.who.int/macrohealth/action/NCMH_Burden%20of%20disease_(29%20Sep%202005).pdf
- Chronic diseases now a leading cause of death in rural India – Mortality data from the Andhra Pradesh Rural Health Initiative. Int J Epidemiol. 2006;35:1522-9.
- [Google Scholar]
- Future Challenges: Thinking Global, Living Local: Voices in a Globalized World. Available from: https://www.futurechallenges.org/local/the-frailty-of-rural-healthcare-system-in-india/
- Prevalence of diabetic nephropathy in an underserved rural community. Indian J Nephrol. 2012;22:484-5.
- [Google Scholar]
- Government of India. Ministry of Home Affairs. The Office of the Registrar General and Census Commissioner. Available from: http://www.censusindia.gov.in/
- [Google Scholar]
- The costs of treating long-term diabetic complications in a developing country: a study from India. J Assoc Physicians India. 2013;61:102-9.
- [Google Scholar]
- Cardiovascular complications of diabetes mellitus in sub-Saharan Africa. Circulation. 2005;112:3592-601.
- [Google Scholar]
- Prevalence of diabetes complications in people with type 2 diabetes mellitus and its association with baseline characteristics in the multinational A1chieve study. Diabetol Metab Syndr. 2013;5:57.
- [Google Scholar]
- Burden of undiagnosed hypertension in Sub-Saharan Africa: a systematic review and meta-analysis. Hypertension. 2015;65:291-8.
- [Google Scholar]
- Social epidemiology of hypertension in middle-income countries: determinants of prevalence, diagnosis, treatment, and control in the WHO SAGE study. Hypertension. 2013;62:18-26.
- [Google Scholar]
- Twenty Eight Community Health Workers Commence Medical Training. Available from: http://www.stabroeknews.com/2011/archives/10/14/twenty-eight-community-health-workers-commence-medical-training%C2%A0/
- [Google Scholar]
- National Health Mission. About Accredited Social Health Activist (ASHA). Available from: http://www.nrhm.gov.in/communitisation/asha/about-asha.html
- [Google Scholar]
- Assessing community health workers' performance motivation: a mixed-methods approach on India's Accredited Social Health Activists (ASHA) programme. BMJ Open. 2012;2:pii: e001557.
- [Google Scholar]




