

Translate this page into:
Acute Ciprofloxacin-Induced Crystal Nephropathy with Granulomatous Interstitial Nephritis
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Crystal-induced acute kidney injury (AKI) is caused by the intratubular precipitation of crystals, which results in obstruction and kidney injury. Ciprofloxacin, a commonly used antibiotic, causes AKI secondary to immune-mediated interstitial injury. Rare mechanisms of ciprofloxacin-induced renal injury include crystalluria, rhabdomyolysis, and granulomatous interstitial nephritis. Clinical and experimental studies have suggested that crystalluria and crystal nephropathy due to ciprofloxacin occur in alkaline urine. Preexisting kidney function impairment, high dose of the medication, and advanced age predispose to this complication. We report a case of ciprofloxacin-induced crystal nephropathy and granulomatous interstitial nephritis in a young patient with no other predisposing factors. The patient responded to conservative treatment without the need for glucocorticoids.
Keywords
Acute kidney injury
ciprofloxacin
crystal nephropathy
granulomatous interstitial nephritis

Introduction
Crystal-induced acute kidney injury (AKI) is caused by the intratubular precipitation of crystals, which results in obstruction and kidney injury. Multiple drugs and toxins are implicated in intratubular crystal-induced obstruction and granulomatous interstitial nephritis. Ciprofloxacin, a commonly used antibiotic causes AKI secondary to immune-mediated interstitial injury. Rare mechanisms of ciprofloxacin-induced renal injury include crystalluria and rhabdomyolysis.[1] Ball found that ciprofloxacin can cause crystal nephropathy in experimental animals.[2] Lien et al.[3] reported the first case of ciprofloxacin-induced granulomatous interstitial nephritis. Very few case reports of ciprofloxacin-induced crystalluria and granulomatous interstitial nephritis have been published worldwide. We report a case of oliguric AKI secondary to ciprofloxacin-induced crystalluria and granulomatous interstitial nephritis.
Case Report
A 25-year-old man, with no comorbidities presented with sudden onset anasarca and oliguria of 2 days duration. He was diagnosed to have hemorrhoids by a local physician and was prescribed oral ciprofloxacin for 5 days with a cumulative dose of 5 g, 10 days before this admission. On investigation, routine blood and urine examination revealed the following results. Hemoglobin 11.7 g/dl, total leukocyte count 5700, neutrophils 80%, lymphocytes 15%, monocytes 3%, eosinophils 2%, platelets 2.2 lakhs/L, S. creatinine 3.6 mg/dl, urea 140 mg/dl, sodium 138 mmol/L, potassium 4.9 mmol/L, chloride 100 mmol/L, calcium 8.5 mg/dl, uric acid 8.0 mg/dl, phosphorus 4.7 mg/dl, total proteins 6.6 g/dl, albumin 3.8 g/dl, serum glutamic oxaloacetic transaminase 21 U/L, serum glutamic pyruvic transaminase 24 U/L, alkaline phosphatase 106 U/L, lactate dehydrogenase 840 IU/L. His urine analysis showed pH of 6.0 and bland sediment without any significant proteinuria, hematuria, eosinophiluria, or leukocyturia. Autoimmune workup including serum rheumatoid factor, antinuclear antibodies, anti-double-stranded DNA, antineutrophil cytoplasmic antibodies did not yield positive results. Serum complement levels were normal. HIV, hepatitis C virus, and hepatitis B virus infections were ruled out. His serum creatinine had increased to 5.8 mg/dl during next 2 days. A percutaneous renal biopsy [Figure 1] was done, which showed ten glomeruli; the glomeruli were unremarkable. Twenty-five percent of tubules shown needle-shaped crystals occupying the entire luminal circumference. These crystals were refringent under polarized light. These intratubular Birefringent crystals [Figure 2] showed a granulomatous response. The granuloma was composed of epithelioid cells. In addition, there was lymphocytic infiltrate in the interstitium. He was managed conservatively with intravenous fluids. His renal function improved during 10 days, and his serum creatinine was 0.9 mg/dl at discharge.

- (a and b) Dense interstitial infiltrate with presence of (c) Interstitial granuloma. (d-f) Presence of intratubular crystals
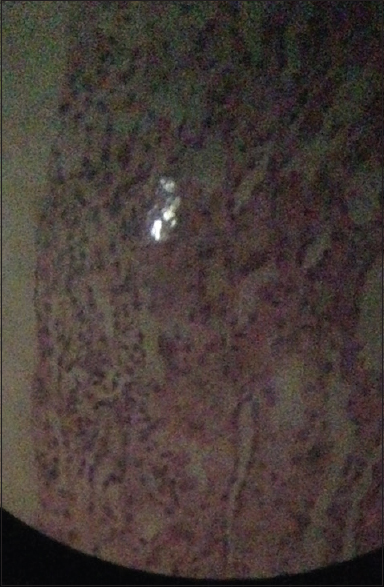
- Birefringent crystals
Discussion
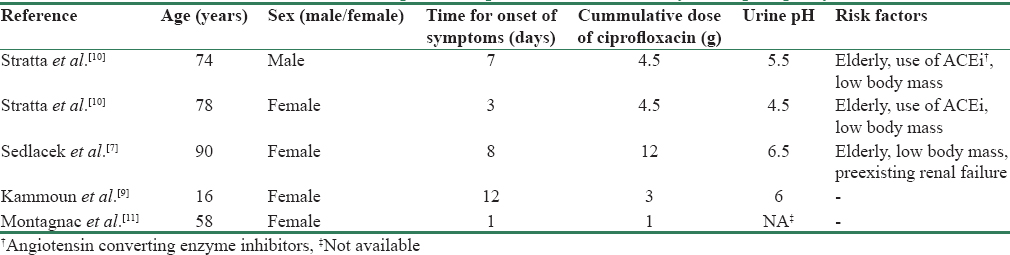
Ciprofloxacin is a commonly used antibiotic that can cause crystal nephropathy as well as granulomatous interstitial nephritis. Crystal-induced AKI most commonly occurs as a result of acute uric acid nephropathy and following the administration of drugs or toxins that are poorly soluble or have metabolites that are poorly soluble in urine.[45] Several commonly used medications such as acyclovir, methotrexate, indinavir, and sulfonamide, are associated with crystalluria and crystal nephropathy. These crystals usually precipitate in distal tubules, obstructs urine flow, and elicits interstitial inflammation. Crystal precipitation depends on the concentration of the drug in urine and urinary pH. Sulfadiazine and methotrexate tend to precipitate in tubule when urine pH is low. Acyclovir intratubular precipitation is increased in alkaline urine. Renal injury due to ciprofloxacin is usually immune mediated. We report a case of ciprofloxacin-induced crystal nephropathy and granulomatous interstitial nephritis. The crystals show a wide array of morphological appearances and precipitates in a urine pH > 6.8. Our patient's urine analysis showed acidic urine without any crystals or casts, unlike alkaline urine pH in which such crystals form. However, the urinary pH is at the time of presentation when the patient had AKI, which may explain the altered pH. The likelihood of occurring AKI in humans with intact tubular function is low.[6] Previous cases have been described after receiving oral ciprofloxacin in a 24-h period or after 8 days of therapy.[78] Our patient presented 10 days after ingestion of ciprofloxacin. Preexisting renal dysfunction, high-dose medication, volume depletion, and old age predispose to this complication.[9] Table 1 shows various published case reports of ciprofloxacin-induced crystal nephropathy. It may be possible that patient had alkaline urine at the time of crystal formation. He did not have any preexisting renal dysfunction and had taken dosage in therapeutic range. It is known that tubular secretion of ciprofloxacin is mediated by organic anion transporters: hOAT3 in basolateral membrane and MRP2 in apical membrane, and that deletion of hOAT3 increases systemic exposure to ciprofloxacin.[12] In our case, it might be postulated that genetic polymorphisms in these transporters lead to systemic accumulation and massive excretion of ciprofloxacin in the renal tubules resulting in development of crystal nephropathy and granulomatous interstitial nephritis. Suma et al.[13] reported crystal nephropathy and granulomatous interstitial nephritis in a 50-year-old male patient after ingestion of twenty tablets of ciprofloxacin. The unique feature of this case report is the occurrence of crystal nephropathy and granulomatous interstitial nephritis with therapeutic dose of ciprofloxacin. The patient responded promptly to withdrawal of ciprofloxacin and conservative treatment. Glucocorticoids and renal replacement therapy may be tried in nonresponding cases. This patient responded to conservative treatment without the need for glucocorticoids. We describe a case of ciprofloxacin-induced crystal nephropathy in young with no associated predisposing factors that can be explained by renal tubular transporter dysfunction.
Conclusion
AKI due to ciprofloxacin may be due to crystal nephropathy and granulomatous interstitial nephritis apart from the usual immune-mediated injury. Conservative measures like adequate hydration may suffice in this condition without any need for steroids.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Rhabdomyolysis and acute renal failure secondary to ciprofloxacin therapy. Therapie. 2012;67:67-8.
- [Google Scholar]
- Ball, Peter. “Ciprofloxacin: An overview of adverse experiences.”. In: Journal of antimicrobial chemotherapy 18. Supplement D (1986). p. :187-193.
- [Google Scholar]
- Ciprofloxacin-induced granulomatous interstitial nephritis and localized elastolysis. Am J Kidney Dis. 1993;22:598-602.
- [Google Scholar]
- Clinical practice. Acute renal colic from ureteral calculus. N Engl J Med. 2004;350:684-93.
- [Google Scholar]
- Crystalluria and ciprofloxacin, influence of urinary pH and hydration. Chemotherapy. 1986;32:408-17.
- [Google Scholar]
- Ciprofloxacin crystal nephropathy – A ‘new’ cause of acute renal failure. Nephrol Dial Transplant. 2006;21:2339-40.
- [Google Scholar]
- Fluoroquinolone induced acute renal failure. General review about a case report with crystalluria due to ciprofloxacin. Nephrol Ther. 2005;1:44-51.
- [Google Scholar]
- Assessment of the role of renal organic anion transporters in drug-induced nephrotoxicity. Toxins (Basel). 2010;2:2055-82.
- [Google Scholar]
- Acute renal failure with ciprofloxacin overdose: Spectrum of renal pathology. Indian Pract. 2015;68:29-31.
- [Google Scholar]




