

Translate this page into:
Kidney Disease in Human Immunodeficiency Virus-seropositive Patients: Absence of Human Immunodeficiency Virus-associated Nephropathy was a Characteristic Feature
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Human immunodeficiency virus (HIV) infection can cause a broad spectrum of renal diseases. However, there is paucity of Indian data on the patterns of renal lesions in HIV-seropositive patients. The aim of the present study was to delineate the spectrum of renal lesions in HIV/acquired immunodeficiency syndrome patients. In this prospective study, all HIV-positive patients of both genders aged >18 years were screened for renal disease. Patients with proteinuria of more than 1 g/24 h were subjected to renal biopsy. A total of 293 HIV-positive patients were screened; of these, 136 (46.4%) patients found to have renal involvement. Dipstick-positive proteinuria of 1+ or more was observed in 112 (38.2%) patients, and 16 (14.2%) patients had proteinuria of more than 1 g/24 h. Renal biopsy in 14 cases revealed glomerulonephritis (GN) in 12 (85.7%) (isolated GN in 4 [28.5%] and GN mixed with chronic TIN in 8 [57.1%]) patients. These include mesangioproliferative GN in 5 (35.7%), membranoproliferative GN in 2 (14.2%), focal segmental glomerulosclerosis in 2 (14.2%), diffuse proliferative GN in 2 (14.2%), and diabetic nephropathy in 1 (7.1%) patients. Chronic interstitial nephritis was noted in 10 (71.42%) (superimposed on GN in 8 [57.1%], isolated in 2 [14.2%]) patients. Granulomatous interstitial nephritis was seen in 3 (24.1%) cases. GN and chronic interstitial nephritis were noted in 85.7% and 71.42% of patients, respectively, mostly superimposed on each other. Mesangioproliferative GN was the most common glomerular lesion, but classical HIV-associated nephropathy was not observed.
Keywords
HIV-associated nephropathy
HIV infection
nephropathies
proteinuria

Introduction
Acquired immunodeficiency syndrome (AIDS) is a disease of the human immune system caused by the human immunodeficiency virus (HIV). Renal disease is a relatively common complication in patients with HIV infection globally, and prevalence of renal disease in HIV patients is about 5–30%.[12] HIV-associated nephropathy (HIVAN) was the first disease to be described in association with HIV infection and reported in the United States in 1984.[3] The spectrum of renal diseases, other than HIVAN, is known to occur in HIV-seropositive patients known as Non-HIV-related kidney diseases. They include HIV-immune complex kidney disease (HIVICK), thrombotic microangiopathy, and combined antiretroviral therapy (cART)-induced nephropathy.[45] The incidence of HIVAN has declined since the introduction of cART, whereas incidence of non HIV-associated chronic kidney diseases (CKD) has increased in post-cART era.[45] The distribution of HIV-associated kidney disease has changed and continued to vary across geographical regions worldwide.[45678] There is paucity of data on histological lesions of kidney in HIV patients from our country. The aim of our study was to analyze the spectrum of histological lesions in proteinuric HIV patients.
Materials and Methods
The study included HIV-seropositive patients of 18 years or above attending antiretroviral treatment (ART) center of our institute between August 1, 2010, and July 31, 2013. The National AIDS Control Organization (NACO) 2007 guideline was used for the diagnosis of AIDS and HIV infection in our study. All patients included in the study were screened for evidence of clinical renal disease using urinalysis, serum creatinine estimation, and ultrasound scan of the kidneys. HIV-positive patients of both genders with clinical renal disease, were subjected to detailed history, physical examination, laboratory investigation including complete blood picture, urine analysis, renal function test, liver function test, random blood glucose, CD4 count, ultrasound of the abdomen, ECG, and chest X-ray PA view. The urine was tested using dipstick method for detection of proteinuria. Those patients having a dipstick proteinuria of 1+ or more were subjected to quantitative 24-h urinary protein estimation. Percutaneous ultrasound-guided kidney biopsy was done in patients with proteinuria of ≥1 g/24 h. Criteria for kidney biopsy were: (1) HIV seropositive, (2) proteinuria of ≥1 g/day, and (3) patients not taking combined antiretroviral therapy (cART) before study. Biopsy was not done in the presence of contraindication or refusal to the procedure. The HIV-positive patients with CD4 lymphocytes count < 350 cells/mm3, and all patients with HIV-associated kidney disease regardless of CD4 lymphocytes count were prescribed highly active antiretroviral therapy (HAART).
The kidney tissue was studied under light microscopy, using hematoxylin and eosin, periodic acid–Schiff, acid fuchsin orange green, and silver stains (for fungus). Electron microscopy and immunofluorescence staining were not done due to lack of facility at our center. Based on standard morphology of the kidney tissue on histological observation, the various spectrums (glomerular and tubular) of kidney lesion were studied in proteinuric seropositive HIV patients.
Results
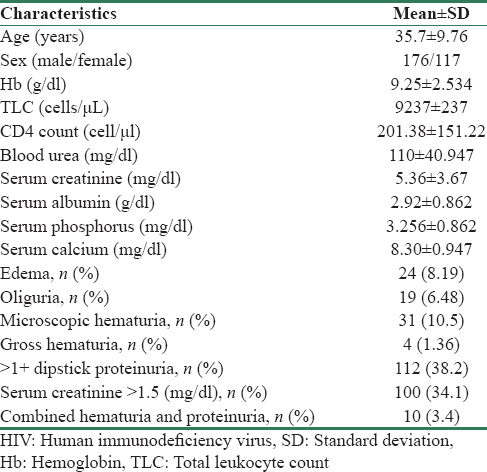
Two hundred and ninety-three (male 176; female 117) HIV-positive patients were recruited in the study. Of 293 patients, 201 had clinical AIDS and 92 cases were HIV positive. The clinical renal disease was noted in 136/293 (46.4%) cases. Dipstick proteinuria of 1+ or more was observed in 112 (38.2%) of patients. Sixteen (14.2%) patients had proteinuria of more than 1 g/24 h. These 16 HIV-positive cases (Male 11 and female 5) were considered for renal biopsy. Kidney biopsy was not done in two cases because of bilateral contracted kidneys [Figure 1]. Thus, renal biopsy was done in 14 patients. Baseline clinical characteristics of HIV patients are shown in Table 1. Most of the patients were anemic (n = 248, 84.78%, as per WHO criteria) with mean hemoglobin value of 9.25 ± 2.53 g/dl. Majority of cases were in advance stages of HIV infection with mean CD4 count of 201.38 ± 151.22 cell/μl, and 180 (61.43%) patients had CD4 count < 200 cell/μl. Renal manifestations of HIV patients include dipstick-positive proteinuria in 112 (38.2%), hematuria in 31 (10.5%), acute kidney injury in 100 (34%), combined hematuria and proteinuria in 10 (3.4%), and oliguria in 19 (6.48%) patients [Table 1].

- The basic plan of study
Quantity of proteinuria in human immunodeficiency virus patients
Twenty-four hours urinary protein estimation was carried out in 112 (38.2%) patients with dipstick proteinuria of 1+ or more. Urinary protein excretion was between 300 and 500 mg/day in 37 cases (33.4%). Eleven patients had proteinuria between 500 mg and 1 g/day (9.8%). We observed proteinuria of 1 g–3.5 g/day in 14 cases (11.8%), and two (1.8%) patients had nephrotic-range proteinuria.
Comparison of clinical parameters between nonproteinuric and proteinuric human immunodeficiency virus-positive patients
The CD4 count was found to be lower in patients with proteinuria (defined as urine dipstick proteinuria of 1+ or more), as compared to those without proteinuria. Similarly, the serum creatinine levels were higher in the proteinuric patients. However, there was no statistically significant difference in CD4 count and serum creatinine level in between the two groups. Although the duration of HIV at the time of presentation was longer in the proteinuric group, there was no statistically significant difference with the nonproteinuric group. Higher percentage (62%) of proteinuric patients were on prescribed HAART therapy in comparison to nonproteinuric patients (44%) at the time of enrollment, which implies patients with high-grade proteinuria have advanced stage of disease in comparison to nonproteinuric patients.
Renal histology
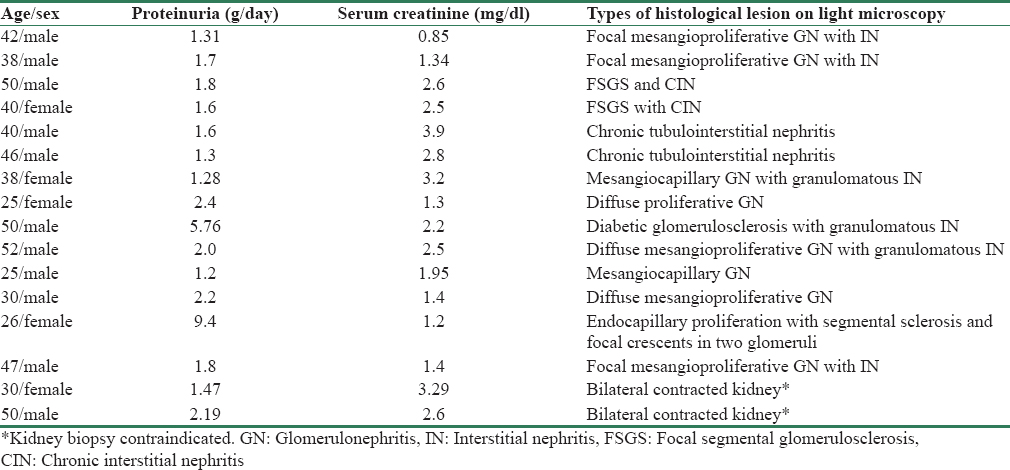
Of 16 HIV-seropositive patients with proteinuria of ≥1 g/24 h; biopsy was done in 14 and 2 cases were excluded from the study because of bilateral small kidneys. The spectrum of renal histological features in 14 patients is shown in Table 2. We noted overall glomerulonephritis (GN) in 12 (isolated 4, mixed lesion: GN combined with interstitial nephritis 8) and chronic interstitial nephritis in 10 (isolated 2; superimposed on GN 8) patients. The most common glomerular lesion was mesangioproliferative GN (n = 5; 31.25%). Focal segmental glomerulosclerosis (FSGS), mesangiocapillary GN, and diffuse proliferative GN were noted in two cases each (n = 2; 12.5%). Diffuse diabetic glomerulosclerosis was noted in one HIV-positive diabetic patient. Chronic tubulointerstitial lesions were seen in 10 (isolated 2; in association with glomerular 8) cases. Granulomatous interstitial nephritis was noted in three cases in association with glomerular diseases. Focal proliferative GN with crescent and focal GBM thickening was observed in one patient. We did not observe classical lesion of HIVAN in our study.
Discussion
AIDS due to HIV infection was first recognized in the United States in 1981.[9] HIV-related renal diseases include various histological spectrum that consists of HIVAN, HIVICK, thrombotic microangiopathy, cART-related nephropathies, and comorbidities-associated nephropathies in HIV patients (such as HCV infection, hypertension, and diabetes).[1011] AIDS-associated nephropathy – known as HIVAN – was first reported in the United States in 1984.[3] HIVAN results from direct viral interaction of renal cells or the action of viral proteins. The characteristic pathological lesion in HIVAN is collapsing FSGS, microcystic tubular dilatation, and endothelial tubuloreticular inclusion on ultrastructural examination.[31213] Mean age of our study population was 35.7 ± 9 years with male and female distribution of 176 and 117, respectively. The higher number of males may be a reflection of higher mobility of this age group in search of livelihood, high sexual activity phase, and to some extent highly emotional and stressful life which usually prevails at this age and sex group. Our finding was in accordance with those from the US and Brazil.[6]
Prevalence of dipstick-positive proteinuria among the HIV-seropositive patients is highly variable in different studies and in different geographical regions. In our study, the prevalence of dipstick proteinuria was 38.2%. Proteinuria was reported in 29.8% and 14% of patients, respectively, in two studies from the USA.[1415] Proteinuria ranged between 6% and 32% in various studies from the USA and Europe.[1617] Reported prevalence of proteinuria in HIV patients was much lower (5–6%) in studies from Africa, Brazil, and Ethiopia.[181920] Range of proteinuria was 17.6%–28% from various Indian studies.[2212223] The proteinuria was noted in 38.2% of cases, and ten patients had active urinary sediments in the present study. Thus, high prevalence of proteinuria in our patients was comparable to other studies.[141623] The higher degree of proteinuria is possibly related to delay in diagnosis, lack of awareness, low education level, and social stigma attached to HIV infection in our study.
HIVAN has been consistently reported to be the most common glomerular lesion in HIV-seropositive patients from the US, Brazil, African countries, and Western Europe.[24] Classic HIVAN histopathology can be seen in adults and children at any stage of HIV infection but is most common in the advanced diseases, including AIDS.[2526] West African descent is highly susceptible to classic HIVAN.[2728] HIVAN has been reported to a lesser degree in Hispanic population and variably in Asian Indian cohort.[192729] However, the disease is notably absent in Swiss–European and Thai population.[30] The current prevalence of HIVAN is declining as result of the widespread use of cART.[31] Without cART, HIVAN progresses rapidly to end-stage renal disease (ESRD). HIVAN was noted in 34% of patients from Chicago.[32] A study from South Africa reported HIVAN in 33% of cases.[33] We have not observed evidence of HIVAN in HIV-infected patients in the present study. In two (14.2%) cases, biopsy evidence of collapsing FSGS was seen, but classic features of HIVAN were absent.[3] In a northern Italian study from three hospitals, no case of FSGS had been found in a large Caucasian cohort.[34] Other studies from Ethiopia and Thailand also could not find any case of HIVAN.[1830] Varma et al. from India did not find any case of HIVAN but reported one case of collapsing FSGS and four cases of noncollapsing FSGS.[21] The first case of classical HIVAN was reported from India in the state of Jammu and Kashmir.[35] Two cases of HIVAN were reported from South India among HIV-infected children presented with nephrotic-range proteinuria.[36] In 2013, Gupta et al.[2] reported collapsing FSGS in 2 of 26 patients, but classical HIVAN was not seen. Even though HIVAN is a rare entity, collapsing FSGS is not uncommon in this part of world.[2]
The most common glomerular lesion was mesangioproliferative GN noted in 5/14 (35.7%) patients. In contrast to our study, mesangioproliferative GN has been reported infrequently from the Western world.[16] No case of mesangioproliferative GN has been reported in the major biopsy series from the United States.[163738] Mesangioproliferative GN was reported in 4/26 (15%) of patients from Italy.[34] A study from South Africa revealed mesangioproliferative GN in 6% of HIV patients.[35] However, a high incidence of mesangioproliferative GN has been reported from other Asian renal biopsy studies. In a series of 26 biopsies in HIV-infected patients in Thailand, mesangioproliferative GN was observed in 65% of the cases.[30] In a study from India, with 25 patients, 8 cases (32%) had mesangioproliferative GN.[21] Similarly, Gupta et al. reported mesangioproliferative GN in 10/26 patients (38.4%)[2] as the most common glomerular lesion. Thus, mesangioproliferative GN is an inconsistent finding in the American, African, and European studies.[343839] However, it represents a dominant renal lesion in HIV-infected individuals in Asia.[22130] However, HIV-associated lupus like GN and thrombotic microangiopathy were not observed in our study.
Epidemiological data showing a decline in the incidence of HIVAN and HIV-associated ESRD in the United States after introduction of cART, suggest that effective control of viral replication can prevent the development of HIVAN.[4041] A study of 221 HIV-positive patients in South Africa reported that both HIVAN and HIVICK showed response to cART.[42] HIV-associated thrombotic microangiopathy also appears to benefit from ART, and a decline in incidence has been reported with widespread ART use.[43] Thus, combined ART has changed the epidemiology of HIV-related kidney diseases. HIVICK and noncollapsing form of FSGS are increasingly reported in the post-cART era.[44] HIVICK is less likely than HIVAN to progress to ESRD and thought to be associated with greater exposure to cART and hepatitis C coinfection.[45] Over the past two decades, a decreasing frequency of classic HIVAN has been observed in African patients living in Europe.[46] cART has been associated with lower incidence of HIVAN, improved kidney function, and lower risk of ESRD in observational studies of patients with biopsy-confirmed or clinically suspected HIVAN. These data reveal that cART seems to have a beneficial role in the prevention and treatment of HIVAN.[44] The HIV Medicine Association of the Infectious Disease Society of America recommended that all patients with HIV-associated kidney disease should receive ART.[47]
Isolated chronic interstitial nephritis was the predominant nonglomerular lesion in our study (15.38%). We observed chronic tubulointerstitial nephritis in association with glomerular lesions in six cases (46%). The granulomatous interstitial nephritis was observed in 23% of patients in association with other glomerular lesions. One of them was secondary to tubercular infection; the etiology of others was unknown. Unlike mesangioproliferative GN, tubulointerstitial diseases have been consistently reported in other studies, but the incidence was low in most of the studies.[163738] However, a high incidence of interstitial nephritis was reported in a multicentric study from Paris; 48% (14/29) in African Americans and 52% (16/31) of Caucasian patients had interstitial nephritis in their series of sixty patients.[48] The prevalence of interstitial nephritis was 20% in another study from India.[21]
Conclusion
The prevalence of dipstick-positive proteinuria in our HIV-seropositive patients was high (38%) and bears no relation to duration of HIV, CD4 count, HAART therapy, and serum creatinine levels. Chronic interstitial nephritis, either in isolation or superimposed on other glomerular lesion, was very common (71%). Mesangioproliferative GN was the most common glomerular lesion similar to other Indian studies. The absence of HIVAN in our HIV patients with proteinuria was a characteristic feature.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Prevalence of renal disease within an urban HIV-infected cohort in Northern Italy. Clin Exp Nephrol. 2014;18:104-12.
- [Google Scholar]
- HIV associated renal disease: A pilot study from North India. Indian J Med Res. 2013;137:950-6.
- [Google Scholar]
- Associated focal and segmental glomerulosclerosis in the acquired immunodeficiency syndrome. N Engl J Med. 1984;310:669-73.
- [Google Scholar]
- Prevalence of chronic kidney disease in Chinese HIV-infected patients. Nephrol Dial Transplant. 2007;22:3186-90.
- [Google Scholar]
- Prevalence of persistent proteinuria in stable HIV/AIDS patients and its association with HIV nephropathy. Braz J Infect Dis. 2007;11:456-61.
- [Google Scholar]
- Renal pathology and premortem clinical presentation of Caucasian patients with AIDS: An autopsy study from the era prior to antiretroviral therapy. Swiss Med Wkly. 2001;131:412-7.
- [Google Scholar]
- Correlation of CD4 counts with renal disease in HIV positive patients. Saudi J Kidney Dis Transpl. 2008;19:603-7.
- [Google Scholar]
- Renal disease in patients with AIDS: A clinicopathologic study. Clin Nephrol. 1984;21:197-204.
- [Google Scholar]
- Glomerular lesions in the acquired immunodeficiency syndrome. Ann Intern Med. 1984;101:429-34.
- [Google Scholar]
- Abnormal urinary protein excretion in HIV-infected patients. Clin Nephrol. 1993;39:17-21.
- [Google Scholar]
- Prevalence of persistent asymptomatic proteinuria in HIV-infected outpatients and lack of correlation with viral load. Clin Nephrol. 2001;55:1-6.
- [Google Scholar]
- Predictors of proteinuria and renal failure among women with HIV infection. Kidney Int. 2002;61:195-202.
- [Google Scholar]
- Is the prevalence of HIV-associated nephropathy decreasing? Am J Nephrol. 1999;19:655-9.
- [Google Scholar]
- Absence of HIV-associated nephropathy in Ethiopians. Am J Kidney Dis. 2006;47:88-94.
- [Google Scholar]
- A cross-sectional study of HIV-seropositive patients with varying degrees of proteinuria in South Africa. Kidney Int. 2006;69:2243-50.
- [Google Scholar]
- Renal disease in an antiretroviral-naïve HIV-infected outpatient population in Western Kenya. Nephrol Dial Transplant. 2007;22:2208-12.
- [Google Scholar]
- Spectrum of renal lesions in HIV patients. J Assoc Physicians India. 2000;48:1151-4.
- [Google Scholar]
- Prevalence of microalbuminuria and proteinuria in patients of HIV/AIDS in Jammu. JK Sci. 2011;13:2.
- [Google Scholar]
- Prevalence of proteinuria and the development of chronic kidney disease in HIV-infected patients. Clin Nephrol. 2004;61:1-6.
- [Google Scholar]
- Human immunodeficiency virus infection and renal failure. Infect Dis Clin North Am. 2001;15:833-50.
- [Google Scholar]
- Human immunodeficiency virus (HIV)-associated nephropathy in children from the Washington, DC area: 12 years’ experience. Semin Nephrol. 1998;18:396-405.
- [Google Scholar]
- Human immunodeficiency virus-associated nephropathy (HIVAN) in Nigerian children. Pediatr Nephrol. 2008;23:117-22.
- [Google Scholar]
- Renal lesions associated with AIDS – An autopsy study. Indian J Pathol Microbiol. 1999;42:63-8.
- [Google Scholar]
- Presentation, pathology, and outcome of HIV associated renal disease in a specialist centre for HIV/AIDS. Sex Transm Infect. 1998;74:179-84.
- [Google Scholar]
- Renal lesions in AIDS: A biopsy and autopsy study. Indian J Pathol Microbiol. 1999;42:45-54.
- [Google Scholar]
- The new epidemiology of HIV-related kidney disease. J AIDS Clin Res (Suppl 4):1. doi: 10.4172/2155-6113.s4-001
- [Google Scholar]
- A spectrum of morphologic lesions of focal segmental glomerulosclerosis by Columbia criteria in human immunodeficiency virus infection. Virchows Arch. 2012;460:429-35.
- [Google Scholar]
- MMed Thesis. University of Witwatersrand; 2014.
- Pattern of glomerular involvement in human immunodeficiency virus-infected patients: An Italian study. Am J Kidney Dis. 1995;26:446-53.
- [Google Scholar]
- Collapsing glomerulopathy in an HIV-positive patient in a low-incidence belt. Indian J Nephrol. 2010;20:211-3.
- [Google Scholar]
- Nephrotic proteinuria and renal involvement in HIV-infected children. Indian J Sex Transm Dis. 2011;32:111-3.
- [Google Scholar]
- Observations on a cohort of HIV-infected patients undergoing native renal biopsy. Am J Nephrol. 2008;28:478-86.
- [Google Scholar]
- Renal disease in an urban HIV population in the era prior and following the introduction of highly active antiretroviral therapy. J Natl Med Assoc. 2011;103:513-7.
- [Google Scholar]
- End-stage renal disease among HIV-infected adults in North America. Clin Infect Dis. 2015;60:941-9.
- [Google Scholar]
- The spectrum of renal histologies seen in HIV with outcomes, prognostic indicators and clinical correlations. Nephrol Dial Transplant. 2012;27:4109-18.
- [Google Scholar]
- HIV-associated thrombotic microangiopathy in the era of highly active antiretroviral therapy: An observational study. Clin Infect Dis. 2004;39(Suppl 5):S267-75.
- [Google Scholar]
- The changing pattern of glomerular disease in HIV and hepatitis C co-infected patients in the era of HAART. Clin Nephrol. 2013;79:285-91.
- [Google Scholar]
- Comparison of risk factors and outcomes in HIV immune complex kidney disease and HIV-associated nephropathy. Clin J Am Soc Nephrol. 2013;8:1524-32.
- [Google Scholar]
- HIVAN is increasingly less common in HIV-positive black Africans living in Europe. Kidney Int. 2006;70:1662.
- [Google Scholar]
- Glomerular dysfunction and associated risk factors over 4-5 years following antiretroviral therapy initiation in Africa. Antivir Ther. 2011;16:1011-20.
- [Google Scholar]
- Renal disease associated with HIV infection: A multicentric study of 60 patients from Paris hospitals. Nephrol Dial Transplant. 1993;8:11-9.
- [Google Scholar]




