

Translate this page into:
A Randomized Controlled Trial of Intravenous versus Oral Cyclophosphamide in Steroid-resistant Nephrotic Syndrome in Children
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
This is a randomized, parallel group, active-controlled trial to compare the efficacy of intravenous cyclophosphamide (IVCP) with oral cyclophosphamide (OCP) in patients with steroid-resistant nephrotic syndrome (SRNS) in children. Fifty consecutive children with idiopathic SRNS were biopsied and then randomized to receive either OCP at a dose of 2 mg/kg/day for 12 weeks or IVCP at a dose of 500 mg/m2/month for 6 months. Both groups received tapering doses of oral steroids. The response was evaluated in terms of induction of complete remission (CR) or partial remission (PR), time to remit, and side effects. The groups were followed up to determine the duration of remission, percentage of patients who remain in sustained remission for more than 1 year after completion of therapy, change in steroid response status, progression to chronic kidney disease stage 3 or more. Of the fifty patients, OCP was given to 25 children and IVCP to 25 children. The demographic data, histopathology, biochemical profile, and duration of follow-up in the two groups were comparable. The rates of induction of CR were 52% versus 44% and of PR were 8% versus 8% in the intravenous (IV) and oral group, respectively. Time to remit was shorter with OCP than IVCP (53 days vs. 84.4 days). Incidence of side effects (both major and minor) was 36% in IVCP versus 20% in OCP group. The actuarial cumulative sustained remission in our study was 12% in IVCP compared with 16% in OCP at 1 year after completion of therapy. Twelve percent children in both the groups exhibited restoration of steroid sensitivity. Thus, in our study, overall, more than half of SRNS patients showed initial response to cyclophosphamide, but only one-fourth patients had sustained remission on follow-up. OCP and IVCP were equally efficacious and safe in idiopathic SRNS in children.
Keywords
Children
cyclophosphamide
India
steroid-resistant nephrotic syndrome

Introduction
Steroid-resistant nephrotic syndrome (SRNS) is a group of heterogeneous diseases characterized by persistence of proteinuria after 4–8 weeks of corticosteroid therapy.[12] Calcineurin inhibitors have a favorable response in SRNS. However, calcineurin inhibitors are expensive, potentially nephrotoxic and need to be continued for a long period of time leading to issues of cost, compliance, and complications. Although generic formulations have decreased the cost of therapy with calcineurin inhibitors the need for prolonged indefinite course, therapeutic drug monitoring, repeat renal biopsies make these drugs beyond the reach of many patients from resource-poor settings. Re-examining the role of less expensive drugs is therefore important.
Cyclophosphamide (CP) is cheap, easily available, has a finite course leading to better compliance, and hence remains an attractive option, especially in developing countries. Although a report from the International Study of Kidney Disease in Children (ISKDC) showed no benefit with oral cyclophosphamide (OCP),[3] results from case series[45] and small trials[67] suggest that it may be an effective therapy, especially in Indian children. A few studies[68] on the subject seem to favor the intravenous (IV) route of administration over oral. This study was undertaken to define the utility of CP in the management of SRNS as well as to assess the efficacy of the oral versus the IV route of administration in these patients.
Materials and Methods
We prospectively studied consecutive patients of SRNS aged between 1 and 15 years, who presented to our nephrology division between January 2008 and June 2011. Informed parental consent and where applicable patient's assent was obtained before starting treatment.
Nephrotic syndrome was defined as the presence of hypoalbuminemia (<2.5 g/dl), proteinuria (>40 mg/m2/h), and edema. Steroid resistance was defined as failure to achieve remission at the end of 4 weeks of treatment with daily prednisolone at the dose of 60 mg/m2. Exclusion criteria included age <1 year, pretreatment with immunosuppressive drugs other than prednisolone in the preceding 6 months, estimate of glomerular filtrate rate (GFR) <60 ml/min calculated from height, and serum creatinine using the Schwartz equation. Patients who developed serious infections such as peritonitis, septicemia, meningitis, septic arthritis, or osteomyelitis more than once during CP therapy were not continued on CP therapy but remained part of the study.
All the study patients underwent a renal biopsy. They were randomized according to random table to receive either intravenous cyclophosphamide (IVCP) (Group 1) or OCP (Group 2). OCP was given in the dose of 2 mg/kg for duration of 12 weeks, and IVCP was administered as pulses of 500 mg/m2/month for six doses. Both groups received alternate day steroids in tapering doses. Patients in IV group received hydration and premedication with ondansetron before CP administration. The drug was dissolved in 250 ml of normal saline and infused IV over 4 h in a supervised day-care setting. Patients were not given mesna.
The children were followed fortnightly during the treatment period. At each visit, the child was evaluated clinically for evidence of disease activity and complications. Complete blood count and urine routine were done fortnightly during the therapy period. Serum albumin, cholesterol, creatinine, urine for spot albumin-creatinine ratio, and 24-h urine albumin were done monthly during the study period. The children were monitored for infections, leukopenia (<4000/μL), and alopecia. When infections or leukopenia were present, the next dose of IVCP was delayed and OCP was withheld until complete normalization of counts or recovery from the infection.
After completion of therapy, children were followed up monthly with clinical and urine examination and 2 monthly with biochemistry and quantification of proteinuria.
Response to therapy
Short-term outcome was assessed at the end of CP therapy in terms of induction of complete remission (CR), partial remission (PR), or no response (NR) [Figure 1]. CR was defined as urinary protein being nil or trace on at least 3 consecutive days or urine protein to creatinine ratio <0.5. PR was defined as urine protein excretion <2+ or urine protein to creatinine ratio between 0.5 and 2 and serum albumin >2.5 g/dl. NR was defined as persistence of 3+ or 4+ proteinuria or urine protein to creatinine ratio >2 (nephrotic range proteinuria). Frequency and severity of side effects were compared in both the groups. Major side effects were defined as those that required hospitalization.

- Comparison of response
Follow-up posttreatment
The mean duration of remission after cessation of treatment was noted in each group. Sustained remission lasting for >1 year or acquisition of steroid-responsive status was considered as favorable outcome. Persistence of proteinuria, development of low GFR (<60 ml/min), end-stage renal disease (ESRD), or death were considered as unfavorable outcomes.
Statistical analysis
Around 15 patients per year fulfilling the case definition could be enrolled, hence a period of 3½ year for enrolling patients. A constraint of sample size due to overall low incidence of SRNS was considered. Randomization was done using random number table. Concealment was done by sequentially numbered, sealed, opaque envelopes. The two groups were compared with respect to intention-to-treat principle. Comparison of variables in both groups was done by Mann–Whitney test and unpaired t-test. Response in both groups was analyzed using Fisher's exact test.
Results
Fifty-five patients with idiopathic SRNS were identified. Two patients were excluded in view of increased serum creatinine at presentation and another three for not giving consent to CP therapy. Data of the remaining fifty patients were used for the purpose of the study [Flowchart 1].
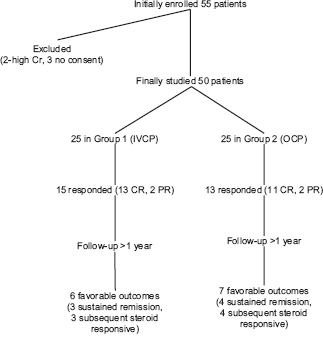
- Study flowchart
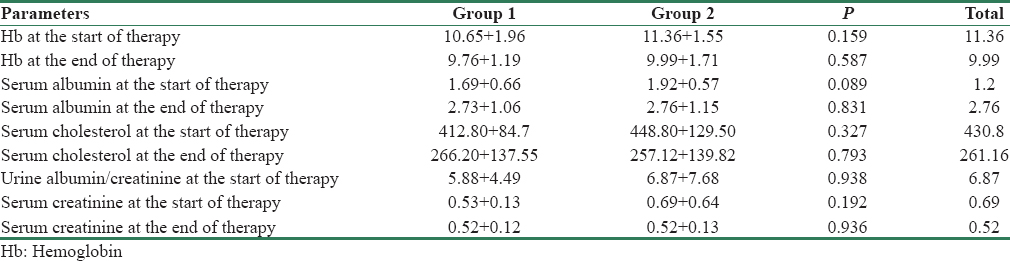
Twenty-five patients were enrolled in each group. Group 1 (IVCP) had 17 males and 8 females whereas Group 2 (OCP) had 14 males and 11 females. Baseline variables such as the age of onset of nephrotic syndrome, serum albumin and cholesterol, severity of proteinuria, and histopathology were comparable between the two groups [Table 1].

Response to cyclophosphamide
In Group 1 (IVCP), 15 of 25 (60%) patients achieved remission. Thirteen achieved CR and two achieved PR. In Group 2 (OCP), 13/25 (52%) achieved remission. Eleven had CR and two PR. The results are comparable (P = 0.076). Time to achieve remission was significantly longer in the Group 1 (86.07 + 29.10 days) as compared to Group 2 (47.45 + 26.06 days) (P = 0.002).
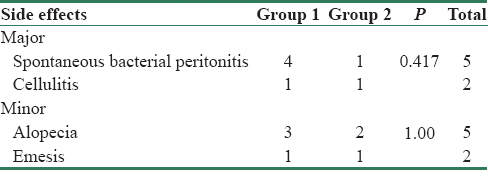
Major side effects were seen in seven patients (14%), five in the Group 1 and two in Group 2. The difference was not significant, P = 0.417. Minor side effects were seen in seven patients; four in Group 1, three in Group 2; which were comparable (P = 1.00). None of the patients required discontinuation of treatment in view of more than two major side effects in the study period. No patient died during the treatment period. None had hemorrhagic cystitis [Table 2]. There was no significant change in hemoglobin or creatinine after CP therapy in either of the two groups (P = 0.587 and 0.936, respectively) [Table 3].
Follow-up posttreatment
The entire cohort was followed up for a mean duration of 17.8 months, 17.72 months in the Group 1, 17.92 in Group 2, which was similar (P = 0.892). Mean duration of remission was similar in both groups 8.13 + 8.85 months versus 9.15 + 8.28 months (P = 0.963). Number of patients who had sustained remission for up to 1 year post cessation of treatment was similar (three patients in Group 1 vs. four patients in Group 2). Restoration of steroid responsiveness was seen in three patients in both the Groups. Four patients progressed to renal insufficiency during the study group (three in Group 2 and one in Group 1) and one patient from Group 2 died of progressive renal failure. One of the patients in renal insufficiency had a familial SRNS. One patient from Group 1 who had a rapid progression to ESRD was transplanted.
Discussion
Studies on the use of CP in SRNS have reported variable response rates ranging from 0% to 70%.[679] Two randomized controlled trials (RCTs) concluded that children with SRNS respond poorly to CP with only 17%–25% of patients achieving remission.[39] The study performed by Tarshish et al. reported that there was no significant difference in the outcome of patients with focal segmental glomerulosclerosis (FSGS) treated with CP (P = 1.00; relative risk [RR], 1.050; 95% CI, 0.75–1.470) as compared to oral prednisolone alone.[3] The ISKDC study, which included children with minimal change nephrotic syndrome (MCNS) and FSGS, reported a somewhat higher CR rate with CP and intermittent prednisolone (56%) than with intermittent prednisolone alone (40%), but there was no significant difference in the long-term outcome between these treatments (P = 0.13; RR, 1.59; 95% CI, 0.58–3.231).[9]
An observational study by Gulati et al. in patients with FSGS treated with IVCP and oral steroids reported CR in 65% and PR in 15% cases.[8] Favorable response to CP has been previously reported from India, irrespective of the underlying histopathology. In a study to consider racial factors on CP sensitivity, 80% of Indian children with SRNS responded to OCP and prednisone (including CR and PR both).[10] High remission rates of 65% were noted with CP in Indian children with FSGS.[11] Histopathological heterogeneity, ethnic differences, and genetic diversity may be responsible for these varied observations.
Three published studies are available comparing the efficacy of OCP versus IVCP [Table 4].

Earlier studies with small number of patients one with 13 MCNS patients and another with 12 FSGS patients found a superior response with IVCP 100% versus 17% in the MCNS study and 40% versus 0% in the FSGS study.[612] A more recent RCT by Mantan et al. included both MCNS and non-MCNS which compared IVCP with OCP found a comparable response with either route of administration. However, their oral arm also had pulses of high-dose IV dexamethasone at periodic intervals.
Our study included patients with both MCNS (58%) and non-MCNS pathology (42%); 26% of our patients had FSGS and 16% mesangioproliferative glomerulonephritis. Overall remission rate with CP was 56% with the majority (48%) achieving CR. The response rates were comparable in both the IV (60%) and the oral group (52%). This is similar to the findings reported by Mantan et al. although we did not use any steroid pulses in the oral arm.
The time to achieve remission in our study was significantly shorter in the oral (47.45 + 26.06 days) as compared to the IV group (86.07 + 29.10 days). The cumulative dosage of CP was significantly lower in the IV group.
Major infectious complications requiring hospitalization were seen in a total of 14% of the children and were comparable in two groups.
Follow-up revealed that 25% of the children who achieved remission had sustained remission lasting >1 year and 21% showed a return of steroid sensitivity. They were equally divided into the oral and IV group. One child developed pulmonary tuberculosis 6 months after omission of CP therapy. Four unresponsive patients, three from the oral group and one from the IV group, progressed to ESRD. One in the oral group had a familial NS.
A limitation of our study was that genetic evaluation was not done, and hence the contribution of genetically mediated resistance to therapy could not be assessed.
Conclusion
Our study shows that CP is a moderately effective drug in the management of SRNS in Indian children and induces remission in half the patients, one fourth of whom maintain remission for more than 1 year. The efficacy as well as the safety was comparable in the oral as well as the IV group. Considering the cost and compliance issues, CP remains an important drug in the setting of SRNS in Indian children in a resource poor setup.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- The primary nephrotic syndrome in children. Identification of patients with minimal change nephrotic syndrome from initial response to prednisone. A report of the International Study of Kidney Disease in Children. J Pediatr. 1981;98:561-4.
- [Google Scholar]
- Prognostic significance of the early course of minimal change nephrotic syndrome: Report of the International Study of Kidney Disease in Children. J Am Soc Nephrol. 1997;8:769-76.
- [Google Scholar]
- Cyclophosphamide does not benefit patients with focal segmental glomerulosclerosis. A report of the International Study of Kidney Disease in Children. Pediatr Nephrol. 1996;10:590-3.
- [Google Scholar]
- Pulse cyclophosphamide for steroid-resistant focal segmental glomerulosclerosis. Pediatr Nephrol. 1999;13:113-6.
- [Google Scholar]
- Intravenous cyclophosphamide in steroid-resistant nephrotic syndrome. Pediatr Nephrol. 2003;18:351-6.
- [Google Scholar]
- Intravenous pulse cyclophosphamide – A new regime for steroid-resistant minimal change nephrotic syndrome. Pediatr Nephrol. 1994;8:1-3.
- [Google Scholar]
- Efficacy of intravenous pulse cyclophosphamide treatment versus combination of intravenous dexamethasone and oral cyclophosphamide treatment in steroid-resistant nephrotic syndrome. Pediatr Nephrol. 2008;23:1495-502.
- [Google Scholar]
- Intravenous pulse cyclophosphamide – A new regime for steroid resistant focal segmental glomerulosclerosis. Indian Pediatr. 2000;37:141-8.
- [Google Scholar]
- Prospective, controlled trial of cyclophosphamide therapy in children with nephrotic syndrome. Report of the International study of Kidney Disease in Children. Lancet. 1974;2:423-7.
- [Google Scholar]
- Steroid-resistant nephrotic syndrome: The influence of race on cyclophosphamide sensitivity. Pediatr Nephrol. 2006;21:1847-53.
- [Google Scholar]
- Steroid-resistant nephrotic syndrome. In: Molony DA, Craig JC, eds. Evidence-Based Nephrology. West Sussex: Wiley-Blackwell; 2009. p. :787-805.
- [Google Scholar]
- Intensive pulse therapies for focal glomerulosclerosis in South African children. Pediatr Nephrol. 1997;11:423-8.
- [Google Scholar]




