

Translate this page into:
IgG4 Disease Diagnosed on Computed Tomography-magnetic Resonance Imaging
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Case Report
A 51-year-old man presented to the emergency department with mild, dull central abdominal pain and dyspepsia for 4 days. There was no history of fever, flank pain, hematuria, or dysuria. There was no history of renal impairment or bowel complaints. His history was significant for diabetes, hypertension, and hyperlipidemia. Abdominal examination revealed soft abdomen with mild generalized tenderness. Laboratory investigation revealed raised serum lipase, amylase levels, along with obstructive jaundice. Urine full examination microscopy elements test and renal function tests revealed no evidence of urinary tract infection. A contrast-enhanced computed tomography (CT) scan of the abdomen and pelvis showed gallbladder wall thickening, biliary dilatation, and swollen pancreas with a subtle lucent halo around the pancreas, associated with mild peripancreatic lymphadenopathy. In addition, there were multiple wedge-shaped areas in both kidneys without any hydronephrosis, nephrolithiasis, or perinephric fat stranding [Figure 1a and b]. Magnetic resonance imaging (MRI) of the upper abdomen confirmed mild edematous pancreatitis and biliary dilation, pancreatic duct dilatation without any ductal calculi. MRI also showed a peripheral halo around the pancreas while diffusion-weighted images demonstrated diffuse restricted diffusion in the pancreas consistent with pancreatitis. MRI evaluation of the kidneys showed multiple T2 dark areas in both kidneys showing restricted diffusion [Figure 2a and b]. These areas were isointense on T1-weighted images, showed progressive enhancement on serial postcontrast images, and again well delineated on 5 min delayed images [Figure 2c–g]. Tumor markers were within normal limits. Endoscopic retrograde cholangiopancreatography showed stricture of the distal common bile duct and pancreatic duct. A biliary stent was placed and biliary brushings were sent for cytology analysis. Endoscopic ultrasound-guided fine needle aspiration cytology (FNAC) was performed sampling the pancreatic head, uncinate process, ampulla, and peripancreatic lymph node. Serum IgG and IgG4 levels performed after CT and MRI were very high. FNAC results showed IgG4 immunostaining of inflammatory cells from the sample from pancreatic head. No malignant cells were seen. A diagnosis of IgG4-related autoimmune pancreatitis, biliary disease, and kidney disease was made. Post-stenting, the markers of obstructive jaundice and pancreatitis went down.

- (a) Axial and (b) coronal contrast-enhanced computed tomography image showing multiple wedge-shaped nonenhancing lesions in both kidneys (arrows) with edematous pancreas associated with a hypodense halo (arrowheads) around it. Note absence of perinephric fat stranding and presence of gallbladder wall thickening
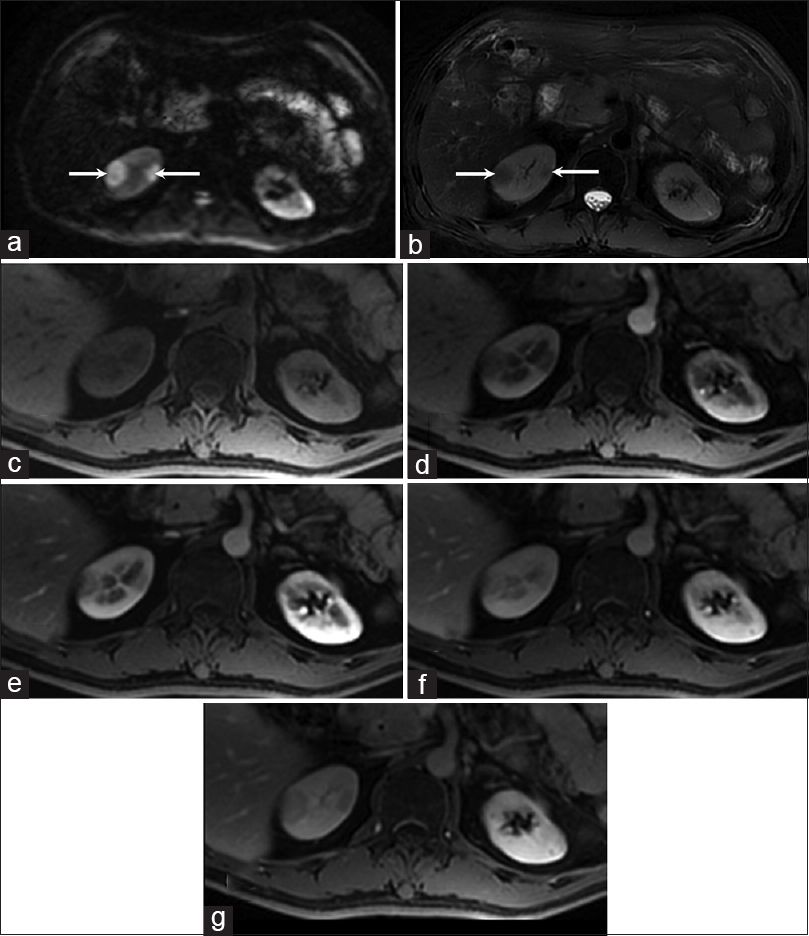
- (a) Diffusion-weighted image (b 1000) showing bright lesions in the right kidney (arrows) that appeared dark on apparent diffusion coefficient map. (b) T2-weighted image shows hypointense lesions in the right kidney (arrows). (c) Unenhanced and serial postcontrast VIBE images (d-f) showing progressively enhancing lesions in the right kidney that become more discrete on 5-min delay image (g)
Discussion
IgG4-related disease is an autoimmune disease that usually affects the pancreas leading to autoimmune pancreatitis. However, it is now well known that this condition can involve kidneys, hepatobiliary system, lymph nodes, salivary and lacrimal glands, gastrointestinal tract, pituitary, and aorta.[1] The IgG4-related disease is characterized by raised serum concentration of IgG4 and infiltration of organs with IgG4-positive plasma cells. IgG4-related kidney disease (IgG4-RKD) is a comprehensive term to describe the renal involvement by the IgG4-positive cells. IgG4-RKD usually affects middle-aged people and in most cases accompanied by the involvement of pancreas or lymph nodes or salivary glands. Tubulointerstitial nephritis is the most common lesion described with IgG4-RKD, but various glomerulonephritis can also be present. CT and MRI findings of IgG4-RKD have been well described.[23] The renal lesions on contrast-enhanced CT appear as nonenhancing small peripheral cortical nodules or cortical wedge-shaped foci of varying sizes. Progressive enhancement in these lesions has also been described. MRI features of the renal lesions are more distinctive. The majority of the renal lesions appear hypointense on T1-weighted, postcontrast T1-weighted, and T2-weighted images and characteristically show restricted diffusion. Radiological differential diagnoses on CT and MRI are pyelonephritis and infiltrative diseases such as amyloidosis and lymphoma. In our patient, the presence of peculiar features of autoimmune pancreatitis associated with typical renal lesions helped in making a diagnosis of IgG-related disease that was subsequently confirmed by serum biomarkers and cytology of the pancreas. This case highlights the imaging features of IgG-RKD and usefulness of important clues for the accurate radiological diagnosis of this rare entity. Physicians and radiologists should be aware of the imaging features so that appropriate treatment (corticosteroids) can be started to prevent further damage to the kidneys.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- IgG4-related kidney disease: MRI findings with emphasis on the usefulness of diffusion-weighted imaging. Eur J Radiol. 2014;83:1057-62.
- [Google Scholar]
- The spectrum of IgG4-related disease in the abdomen and pelvis. AJR Am J Roentgenol. 2013;201:14-22.
- [Google Scholar]




