

Translate this page into:
Lymphorrhea: An Unusual Complication of Jugular Venous Catheterization for Hemodialysis
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
A considerable number of end-stage renal disease patients undergo tunneled cuffed catheter insertion for hemodialysis under ultrasonographic guidance while awaiting arteriovenous fistula creation. We report a case of a 62-year-old female who underwent tunneled catheter insertion in the left internal jugular vein under ultrasound and fluoroscopic guidance, which was followed by pericatheter serous discharge. Fluid examination confirmed the diagnosis of lymphorrhea, and lymphoscintigraphy facilitated its localization. This case is reported for its rarity and with a discussion on literature review, complications of lymphorrhea, and their management.
Keywords
Lymphorrhea
lymphoscintigraphy
tunneled hemodialysis catheterization

Introduction
Trauma of adjacent structures is a well-known potential complication of tunneled cuffed catheter (TCC) insertion. Use of real-time ultrasound (US) guidance has decreased the rate of complications and improved the initial technical success rates.[1] Lymphatic disruption has been frequently reported, complicating the insertion of central lines,[23] pacemakers,[4] and thoracic and neck surgeries (chylous fistula occurring in 1%–2% of comprehensive neck dissections[5]) but has been rarely reported with hemodialysis (HD) catheters.[67] We report a rare case of lymphorrhea complicating insertion of left internal jugular vein (IJV) TCC insertion under US guidance, which was managed without catheter removal.
Case Report
A 62-year-old (body mass index 28.2 kg/m2), hypertensive, and nondiabetic female patient with end-stage renal disease (ESRD) secondary to crescentic glomerulonephritis was on maintenance HD since the last 8 years through the right-sided brachiocephalic fistula. She presented with brachial artery aneurysm and underwent closure of arteriovenous fistula (AVF). Insertion of the left IJV TCC was planned as the right IJV was not patent. After local preparation, the left IJV was cannulated under ultrasonographic guidance in single prick. The position of guide wire was confirmed fluoroscopically. A subcutaneous tunnel was created over the left anterior chest wall using a malleable tunneler. Exit site was approximately 5 cm below the clavicle; the tunnel was well above the breast tissue. Entry site was serially dilated to allow the insertion of 15F PTFE introducer with a peel-away sheath, which went in effortlessly. A 14.5 Fr, cuffed polyurethane catheter (Bard Hemosplit®: Bard Access Systems, C.R. Bard Inc.,) was inserted through the sheath, and tip placement was confirmed by fluoroscopy. There was free backflow of venous blood through both the ports. Hemostasis was achieved followed by dressing of entry and exit site. After 8 hours, serous discharge was observed from the venotomy site, which progressively became copious causing soakage of 6–7 gauze pieces every hour. 2 ml of milky fluid was aspirated from the puncture site [Figure 1]. Microscopic examination was remarkable for lymphocytic preponderance. Biochemistry showed protein concentration 2.64 g/dl, cholesterol 560 mg/dl, triglycerides 915 mg/dl, and presence of chylomicrons. Computed tomography (CT) scan of chest confirmed the catheter tip in the superior vena cava through the brachiocephalic vein and showed no collection around the catheter or in the thoracic cavity. 99mTc-labeled nanocolloid lymphoscintigraphy with single-photon emission CT-CT (SPECT) correlation was done, which revealed tracer accumulation at the left supraclavicular region near the dialysis catheter confirming the diagnosis of chyle leak [Figure 2]. The patient underwent her scheduled HD after 18 h with blood flow up to 300 ml/min. As there was no catheter dysfunction and it was a precious access (opposite IJV blocked, no potential veins for AVF), it was decided to conserve the catheter. Purse-string sutures were taken at the venotomy site and compression dressing done. The patient was given 45° propped up position and was kept on a high protein, low-fat diet. During next 48 h, the chyle leak decreased, however did not stop. The patient's blood pressure fell down from 150/90 to 100/50 mmHg; all her antihypertensive drugs were withdrawn. Her central venous pressure was low, capillary refill time was more than 5 s, and serum albumin dropped from 4.1 to 2.8 g/dl. She was given infusion of 20% human albumin, and fluid intake was increased to maintain euvolemia. She developed leukocytosis (total lymphocyte count 19,600/mm3), which could be an inflammatory response as she remained afebrile; she was treated with empirical intravenous antibiotics, which were stopped once blood cultures were documented sterile. Over the next 4 days, leak progressively decreased and her blood pressure improved. Once stable, the patient was discharged with advice to continue the maintenance HD through the same catheter. The patient has been on regular outpatient department follow-up since the last 8 months and is adequately dialyzed with the same catheter.

- Discharge from the venotomy site in the left supraclavicular fossa. Insert: milky fluid aspirated from skin surface in the syringe before sending for investigation
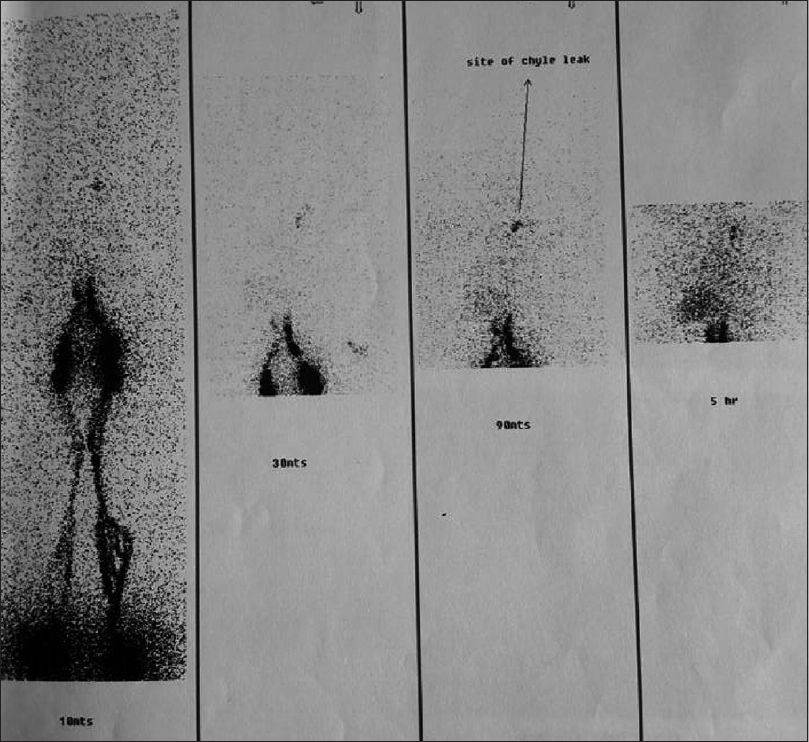
- 99mTc-labeled lymphoscintigraphy with single-photon emission computed tomography-computed tomography localizing the site of the lymph leak
Discussion
Injuries to structures in the vicinity are possible complications of IJV cannulation, one of which being lymphatic disruption. In the superior mediastinum, the thoracic duct crosses anterior to subclavian and vertebral arteries and posterior to the left carotid artery and left IJV. At termination, it opens into the angle between the junction of left subclavian vein and IJV, either as a single duct or double/triple endings, or can also end into the left subclavian, IJV or innominate vein.[8] Furthermore, instead of the usual termination at the posterolateral aspect of the venous angle, anterolateral termination can occur.[8] These variations pave the way for inadvertent lymphatic disruption, likelihood of which increases with history of multiple catheter placements, more needle passes, difficulty in proceeding the guide wire,[2] and in patients with severe pulmonary hypertension.[3] However, in our case, none of the above factors were present. Our catheter was inserted under real-time US guidance, and the position was fluoroscopically confirmed. Most probable cause of the lymphatic leak in our patient appears to be trauma to the thoracic duct either while it is anterolateral to the vein (which becomes more anterior when the head is rotated to contralateral side) or at its termination at the confluence of the left subclavian vein and IJV. Routine use of chest X-ray/fluoroscopy has been advocated to detect catheter tip malposition; however, both were unremarkable in our case. Use of 99mTc-labeled lymphoscintigraphy coupled with CT helps in diagnosis and in anatomic localization of lymph leak.[9] Thus, we recommend the use of lymphoscintigraphy to detect the exact location of lymphorrhea, and this can also guide embolization in refractory cases.[5] Due to their role of transporting lipids and proteins to the systemic circulation, lymphatics play a crucial part in fluid homeostasis and preventing malnutrition. Hypoproteinemia and hypotension found in our patient, which responded to albumin infusion, point toward the need for prompt fluid resuscitation in cases of lymphorrhea. Furthermore, lymph being rich in T lymphocytes also has an immunological role and sepsis has been described in patients with lymphorrhea; thus as our patient developed leukocytosis, she was treated with prophylactic antibiotics. The management of lymphorrhea includes nursing in a semi-erect position with high protein diet, which contains medium-chain triglycerides as the sole source of fat. Refractory cases may mandate infusion of somatostatin[10] and infusion of a sclerosing agent.[5] In 25%–50% of cases, local tamponade effect due to collection of lymph with blood may seal the defect spontaneously, but occasionally, the use of positive pressure ventilation is warranted.[10] Finally, either surgical ligation of lymphatics or percutaneous transabdominal thoracic duct catheterization and embolization[11] may be required. Majority of the reported cases were managed with removal of the catheter[67] which becomes challenging in ESRD patients with limited access options. Our patient highlights the fact that lymphorrhea can be managed without sacrificing the catheter; however, this practice cannot be universally acceptable and the decision to remove the catheter should be individualized.
Conclusion
Interventional nephrologists should be aware of potential anatomic variations in the lymphatics and their plausible disruption during placement of HD catheters. If lymphorrhea occurs, prompt attempts must be made to control it and to replace the volume loss with appropriate fluid resuscitation. Furthermore, it is prudent to carefully monitor hemodynamics and to ensure adequate nutrition in cases of chronic lymphorrhea.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We acknowledge the patient, her relatives, and our nursing staff assisting the procedure.
References
- Insertion of internal jugular temporary hemodialysis cannulae by direct ultrasound guidance – A prospective comparison of experienced and inexperienced operators. Clin Nephrol. 1998;50:320-5.
- [Google Scholar]
- An unusual complication of central venous catheterization. CHRISMED J Health Res. 2015;2:276.
- [Google Scholar]
- Lymphatic leak complicating central venous catheter insertion. Cardiovasc Intervent Radiol. 2005;28:839-40.
- [Google Scholar]
- Damage to right lymphatic duct. A complication of temporary pacemaker insertion. Anaesthesia. 1984;39:254-6.
- [Google Scholar]
- Modern management of chylous leak following head and neck surgery: A discussion of percutaneous lymphangiography-guided cannulation and embolization of the thoracic duct. Otolaryngol Clin North Am. 2008;41:1231-40. xi
- [Google Scholar]
- Lymph leakage following subclavian vein catheterization. Nephrol Dial Transplant. 1999;14:447-8.
- [Google Scholar]
- Lymphorrhea following percutaneous right supraclavicular hemodialysis catheter placement. Nephron. 1993;64:500.
- [Google Scholar]
- A morphological study of the thoracic duct at the jugulo-subclavian junction. J Craniomaxillofac Surg. 1999;27:100-4.
- [Google Scholar]
- Lymphoscintigraphy using (99m)Tc filtered sulfur colloid in chylothorax: A case report. J Nucl Med Technol. 2001;29:30-1.
- [Google Scholar]
- Thoracic duct injury associated with left internal jugular vein catheterization: Anatomic considerations. J Vasc Interv Radiol. 2002;13:337-9.
- [Google Scholar]
- Management of chylothorax by percutaneous catheterization and embolization of the thoracic duct: Prospective trial. J Vasc Interv Radiol. 1999;10:1248-54.
- [Google Scholar]




