

Translate this page into:
De-Novo Focal Crescentic IgA Nephropathy in a Renal Allograft Recipient
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Sir,
IgA nephropathy (IgAN), the most common type of glomerulonephritis (GN), can recur in an allograft in up to 60% of patients[1] and could lead to allograft loss in approximately 16% of such cases.[2] Crescentic IgAN accounts for one third of cases of immune complex crescentic GN in native kidneys.[3] De-novo IgAN with focal or diffuse crescents in transplanted kidneys are extremely uncommon.[4]
A 46-year-old hypertensive male, recipient of a live renal allograft before 7 years, presented with acute onset of fever, swelling, and pain in the left lower limb following a trauma. His primary renal disease leading to chronic kidney disease was clearly not known. Over the last 7 years, allograft function was stable with a serum creatinine (Sr. Cr) of 1.1 mg/dL with normal urine sediments. Furthermore, he did not have a history of acute rejections or previous renal allograft biopsies. His current immunosuppressive drugs consisted of prednisolone (5 mg/day), tacrolimus (trough level maintained between 3 and 5 ng/mL), and mycophenolate mofetil (1 g/day).
During this admission, the patient had leucocytosis, acute graft dysfunction (Sr. Cr: 1.6 mg/dL), microscopic hematuria, and left lower limb cellulitis. He had 2.8 gm proteinuria with serum albumin of 3.4 g/dL. Renal ultrasound and serum complement levels were in normal range and blood and urine cultures were sterile. He was started on intravenous antibiotics; cellulitis was confirmed on the limb ultrasound and was advised for conservative approach by the attending surgical team. Over the next 3 days, his Sr. Cr increased to 2.7 mg/dL and the patient underwent a renal allograft biopsy. On light microscopy (LM), three out of seven glomeruli had cellular crescents with mild mesangial expansion without endocapillary hypercellularity and necrosis. The basement membrane was single contoured without evidence of thickening [Figure 1a and a]. There was no histological evidence of acute rejection. On immunohistochemistry (IHC), C4d staining was negative. His serum anti-nuclear antibody, anti-neutrophil cytoplasmic antibody, and anti-glomerular basement membrane antibody were negative.
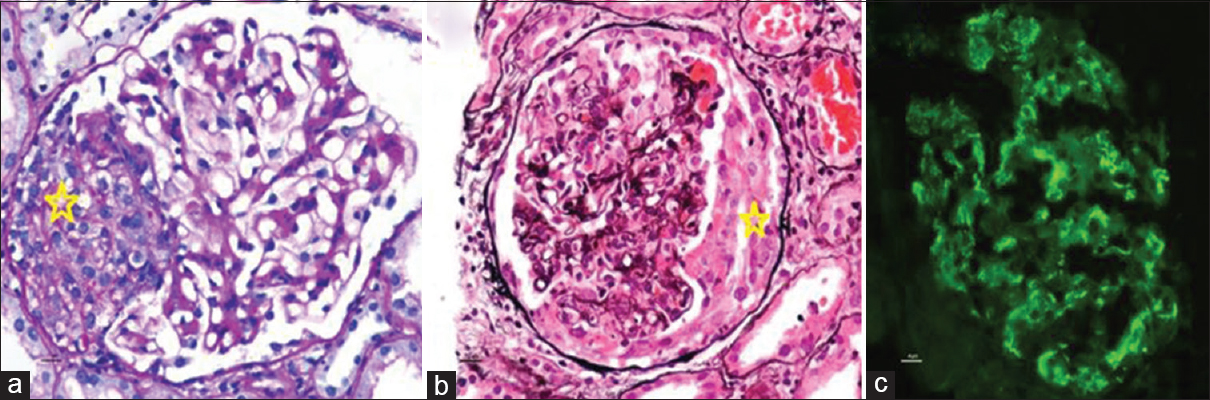
- *Crescents; (a) Hematoxylin and Eosin stain × 40; (b) PAS stain × 40; (c) immunoflourescence IgA stain
With histological diagnosis of focal crescentic mesangioproliferative GN, the patient was treated with a single dose of pulse methylprednisolone (500 mg) under antibiotic cover. His maintenance dose of steroid was increased to 0.5 mg/kg/day. Patient's renal function improved over the next 1 week. A repeat renal allograft biopsy after 2 weeks showed reduced number of crescents (1 out of 8 glomeruli). On immunofluorescence (IF), there was diffuse and global granular deposits of IgA (3+) and C3 (1+) in the mesangium while IgG, IgM, and C1q staining were negative [Figure 1c]. Patient's steroid dose was gradually tapered to 10 mg/day over the next 4 weeks. His renal functions remained stable at 1 year of follow-up and his Sr. Cr was 1.2 mg/dL.
Our case of late-onset de novo focal crescentic IgAN in a patient with preceding lower limb cellulitis showed favorable outcome with aggressive management. Previously, Tang et al.[5] and Kowalewska et al.[4] reported three cases each of recurrent crescentic IgAN. The extent of glomerular involvement by these crescents ranged from 6.9% to 30%.[4] De novo occurrence of focal crescentic IgAN in renal allograft following infection has not been previously reported. Infection-related GN (IRGN) with predominant IgA deposits are often reported in elderly patients, but the lack of proliferative nature of glomeruli and absence of positive culture for staphylococcus aureus with normal serum complement levels in this patient ruled out IRGN. Furthermore, our patient underwent an allograft biopsy in view of deteriorating allograft function with a suspicion for rejection. Biopsy showed focal crescentic GN (crescents 43%) with mesangial expansion and IgA deposits, confirmed on subsequent biopsy. Since this patient's primary renal disease was suspected to be interstitial disease, renal tissue was not sent for IF examination in the initial renal allograft biopsy. IgAN in the renal allografts with the epithelial crescent formation is an uncommon and aggressive form of a disease that can occur at any time during the post-transplant period. This often follows an aggressive clinical course and leads to subsequent allograft loss.[4] Allograft function improved in our patient with pulse steroids, administered under the cover of intravenous antibiotics which aided in resolution of cellulitis. Histologically, there was a reduction in the number of crescents (12.5%) on subsequent biopsy. The resulting bacteremia following skin infection – subsequent superantigen-induced polyclonal antibody production with the formation of antigen, IgA complexes, and deposition of these complexes in the glomerulus – has been the proposed mechanism for IgAN following cellulitis.[6]
De novo IgAN can occur following systemic infection in renal allograft recipients. Physicians should have a low threshold for allograft biopsy and tissue should always be processed for complete IF study especially in the presence of proteinuria and active urine sediment. The prognosis for the disease is good with a resolution of the primary triggering event.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that his name and initials will not be published and due efforts will be made to conceal his identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Recurrent IgA nephropathy after renal transplantation. Semin Nephrol. 2004;24:287-91.
- [Google Scholar]
- Glomerulonephritis recurrence in the renal graft. J Am Soc Nephrol. 2001;12:394-402.
- [Google Scholar]
- IgA nephropathy with crescents in kidney transplant recipients. Am J Kidney Dis. 2005;45:167-75.
- [Google Scholar]
- Recurrent or de novo IgA nephropathy with crescent formation after renal transplantation. Ren Fail. 2008;30:611-6.
- [Google Scholar]
- IgA dominant post-infectious glomerulonephritis: Pathology and insights into disease mechanisms. Diagnostic Histopathol. 2013;19:175-81.
- [Google Scholar]




