

Translate this page into:
Non Obstructive Hydrocolpos Due to Vesicovaginal Reflux in an Adolescent Female
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 14-year-old, adolescent female was referred to the Department of Imaging for pelvic ultrasonography with complaints of recurrent urinary tract infections since childhood which had increased in frequency over the course of last 6 months. Patient was obese (weight: 72 kg and height: 1.6 m (body mass index = 28.12 kg/m2)). Menstrual history was unremarkable and clinical examination revealed normal external genitalia. Internal examination was not performed as the patient did not consent for the same. Renal function tests and blood counts were in the normal range. Urine microscopy revealed pus cells, epithelial cells, and gram-negative bacteria. Urine culture revealed Escherichia coli. Ultrasonography revealed an anechoic lesion posterior to the distended urinary bladder causing its anterior displacement with posterior acoustic enhancement. It was causing superior displacement of the uterus and outlining the cervical os [Figure 1a], therefore, consistent with a fluid-filled vagina (hydrocolpos). Uterus, bilateral ovaries, and urinary bladder were normal. The post-void scan revealed complete resolution of the hydrocolpos, suggesting a plausible diagnosis of vesicovaginal reflux [Figure 1b]. Thereafter, Magnetic Resonance Imaging (MRI) of the pelvis was done which revealed distended fluid-filled vagina on full bladder imaging suggestive of hydrocolpos [Figure 2a]. Mass effect due to hydrocolpos was noted on the adjacent structures like urinary bladder and uterus. The post void MRI revealed resolution of the fluid-filled vaginal distension [Figure 2b]. There was no evidence of an ectopic ureter, vesicovaginal fistula, bladder diverticuli or any other structural abnormality, thereby cementing the diagnosis of non-obstructive hydrocolpos due to vesicovaginal reflux. The patient was advised to undergo behavioral therapy with a voiding retraining program, including the proper toileting position, as a part of her management.

- Pelvic ultrasonography in prevoid (a) and post void (b) states using low frequency (3-5 MHz) transducer showing anechoic lesion (black arrow) seen posterior to the distended urinary bladder causing its anterior displacement, posterior acoustic enhancement, outlining the cervical os and causing superior displacement of the uterus consistent with hydrocolpos. The post-void scan revealed complete resolution of the hydrocolpos (white arrow), suggesting a plausible diagnosis of vesicovaginal reflux
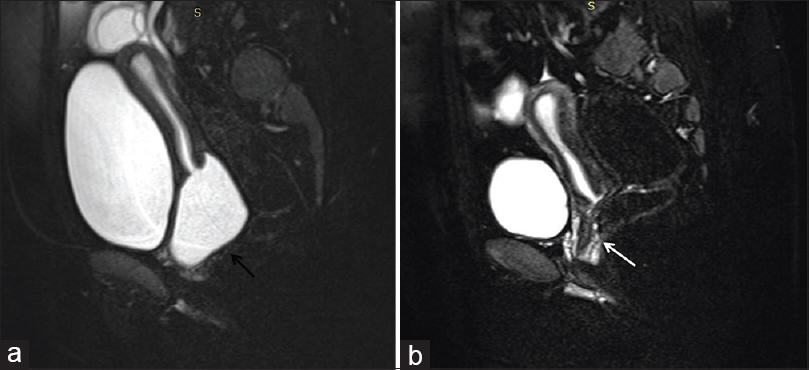
- Sagittal T2 weighted sections of MRI pelvis with fat suppression in prevoid (a) and post void (b) states. Distended fluid-filled vagina on full bladder imaging representing hydrocolpos (black arrow) with mass effect on the adjacent structures like urinary bladder and uterus. The post void MRI revealed resolution of the fluid-filled vaginal distension (white arrow). No structural abnormality was demonstrable on MRI
Hydrocolpos refers to the dilatation of vagina due to fluid, which could be cervical or endometrial secretions or rarely urine. Etiology is either obstructive (transverse vaginal septum, imperforate hymen, vaginal atresia, vaginal agenesis) or non-obstructive (misplaced bladder catheter, vesicovaginal reflux, leakage of amniotic fluid in pregnant patient).[1] Vesicovaginal reflux (VVR) though a common entity, is an uncommon cause of hydrocolpos. VVR is a functional voiding disorder which falls under the umbrella of a spectrum of diseases referred to as dysfunctional elimination syndrome. VVR has variable clinical presentation ranging from asymptomatic bacteriuria, enuresis to vulvovaginitis.[23] Etiology of VVR is unclear with a few predisposing factors being implicated: Obesity with tightly opposed large labia majora which prevent passage of urine, abnormal toileting position with voiding with legs apposed tightly, adhesions of labia minora, ureteral duplication or ectopic ureter with insertion into vagina, female hypospadias, spastic pelvic floor muscles due to functional disorder or cerebral palsy.[1] VVR is rarely encountered in radiological literature because of it predominantly being a clinical diagnosis. Treatment is behavioral therapy with a voiding retraining program.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Vesicovaginal reflux mimicking obstructive hydrocolpos. J Ultrasound Med. 2007;26:1781-4.
- [Google Scholar]
- Vesicovaginal reflux: Recognition and diagnosis using ultrasound. Pediatr Radiol. 2010;40:114-7.
- [Google Scholar]




