

Translate this page into:
Neck Lump Unmasking Multiple Myeloma in a Patient with Acute Kidney Injury
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Extramedullary plasmacytomas commonly occur in the upper aerodigestive tract. Most plasma cell neoplasms of the larynx represent solitary extramedullary plasmacytomas without multiple myeloma (MM). Thyroid cartilage infiltration in MM is very rare. Here, we describe a patient who presented with a neck lump. Further evaluation revealed plasmacytoma of thyroid cartilage secondary to indolent MM with associated hypercalcemia and acute kidney injury (AKI), which recovered spontaneously with conservative therapy.
A 59-year-old man presented with neck lump and hoarseness of voice for 2 months. On examination, there was swelling in the middle of neck anteriorly, moving with deglutition. Direct laryngoscopy showed extrinsic laryngeal mass with displacement of vocal cords resulting in narrowing of glottis. Laboratory evaluation revealed pancytopenia (hemoglobin- 6.0 g/dL, white blood cells- 3.5 × 103/μL, and platelets- 103 × 103/μL), hypercalcemia (corrected calcium- 14.2 mg/dL), hyperuricemia (uric acid- 11.8 mg/dL), and renal dysfunction (urea- 136 mg/dL, creatinine- 5.2 mg/dL) with euthyroid status. PTH was suppressed, and 25-hydroxy vitamin D3 was normal. Serum proteins showed reversal of albumin: globulin ratio (total proteins- 9.9 g/dL, albumin- 3.9 g/dL, globulins- 6.0 g/dL). Erythrocyte sedimentation rate (ESR) was 84 mm/h. He also had non-albumin proteinuria (high spot urine protein to creatinine ratio [4 g/g] with trace albumin on urine dipstick). Neck imaging showed a large lobulated mass involving the thyroid cartilage, causing its destruction with displacement of the vocal cords [Figure 1a]. Fine-needle aspiration cytology from thyroid cartilage mass suggested a plasma cell neoplasm [Figure 1b]. Further evaluation with serum protein electrophoresis (M band [3.01 g/dL] in beta region), immunofixation (monoclonal gammopathy in IgA and κ light chain region), and serum free light chain assay (κ- 4070 mg/L, λ- 20.3 mg/L; κ:λ ratio- 154.75) suggested underlying MM of IgA, κ type. Skeletal survey showed multiple lytic lesions of the axial skeleton. Bone marrow biopsy confirmed the diagnosis of MM with 70%–80% atypical plasma cells [Figure 1c]. Myeloma cytogenetics by fluorescence in situ hybridization is awaited. Serum beta-2 microglobulin was 31.7 mg/L, albumin was 2.9 g/dL, and lactate dehydrogenase (LDH) was 320 U/L. Our patient also satisfied nearly all the criteria of myeloma-defining events; (CRAB [hypercalcemia, renal dysfunction, anemia, and lytic bone lesions], clonal bone marrow plasma cells ≥60%, involved: uninvolved serum freelight chain ratio ≥100, and more than one focal lesion on magnetic resonance imaging, with each focal lesion ≥5 mm). He was managed with hydration, corticosteroids, denosumab, and chemotherapy (cyclophosphamide, bortezomib, and dexamethasone [CyBorD or VCD]). His azotemia and hypercalcemia showed gradual recovery. Thus, the diagnosis of plasmacytoma of thyroid cartilage secondary to MM was made.
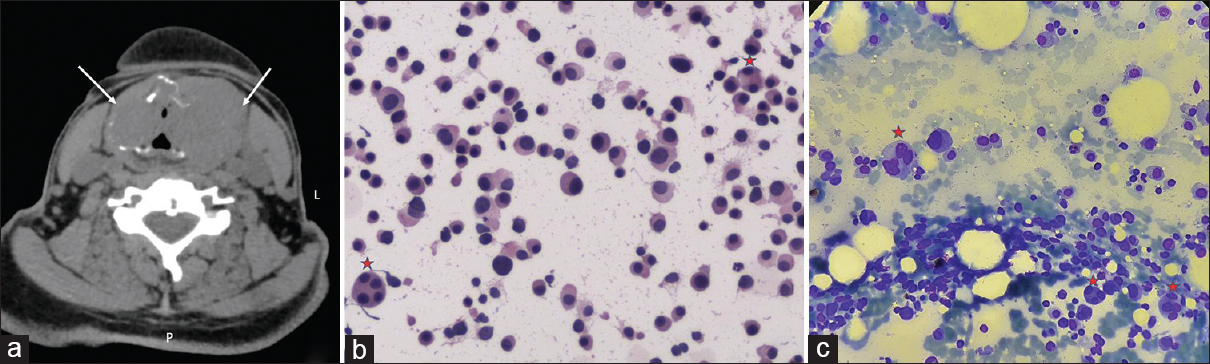
- (a) Plain CT scan neck, axial section showing a large lobulated isodense lesion (6.9 × 4.5 cm) involving the thyroid cartilage (arrows), causing its destruction with compression and displacement of the vocal cords medially, resulting in luminal narrowing at the level of glottis. (b) FNAC from thyroid cartilage mass showing diffusely scattered cells mostly consisting of plasma cells and few lymphocytes. Few plasma cells show binucleated and multinucleated forms (*). The cells show moderate amount of amphophilic cytoplasm with dark round eccentric nuclei. These features are consistent with plasma cell neoplasm (hematoxylin and eosin stain, ×20). (c) Bone marrow aspiration smear showing hypercellular marrow containing predominantly plasma cells (70%–80%) with markedly decreased normal marrow elements. The plasma cells show abundant cytoplasm and large eccentric vesicular nucleus, with perinuclear halo, and few show prominence of nucleoli. Few binucleated and multinucleated plasma cells are seen (*) (Giemsa stain, ×40) CT = computed tomography, FNAC = fine-needle aspiration cytology
Plasmocytomas can be solitary and localized (either bone or extramedullary) or associated with MM. Extramedullary plasmacytomas are very rare (<5% of all plasma cell neoplasms) and commonly occur in the upper aerodigestive tract.[1] They are benign and localised, but around 50%–60% progress to MM. Most plasma cell neoplasms of the larynx represent solitary extramedullary plasmacytomas without MM, rather than extraosseous MM.[2] Thyroid cartilage infiltration in MM is very rare. All the cases of plasmacytoma need to be evaluated thoroughly in order to distinguish solitary bone or extramedullary plasmacytoma from MM for prognostic and therapeutic implications, as localized radiotherapy or surgery is preferred in the former and systemic chemotherapy ± autologous stem cell transplantation in the latter. The two mechanisms suggested for cartilaginous involvement in MM are (a) direct extension from adjacent plasmacytoma and (b) metaplasia of cartilage to bone with the formation of marrow cavity, in which plasma cell proliferation takes place.[3] AKI in our case could be multifactorial due to dehydration, hypercalcemia, and with the possibility of cast nephropathy. Kidney biopsy was not performed as renal function showed spontaneous recovery with reduction in calcium levels and bortezomib-based chemotherapy. This case illustrates that a destructive laryngeal plasmacytoma can rarely be the sole clinical manifestation of underlying indolent MM with associated hypercalcemia and AKI.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Multiple myeloma involving the thyroid cartilage. Auris Nasus Larynx. 2007;34:277-9.
- [Google Scholar]
- Multiple myeloma involving the thyroid cartilage: case report. Am J Neuroradiol. 2002;23:316-8.
- [Google Scholar]
- An indolent course of multiple myeloma mimicking a solitary thyroid cartilage plasmacytoma. Eur Arch Otorhinolaryngol. 2002;259:84-6.
- [Google Scholar]




