

Translate this page into:
Auricular Chondritis and Renal Medullary Angiitis – An Uncommon Manifestation of Antineutrophilic Cytoplasmic Antibody Associated Vasculitis
Corresponding author: Aman Jha, Department of Nephrology, Asian Institute of Gastroenterolgy Hospitals, Hyderabad, Telangana, India. E-mail: amanjha14927.aj@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Jha A, Madireddy N, Jha R, Gowrishankar S. Auricular Chondritis and Renal Medullary Angiitis – An Uncommon Manifestation of Antineutrophilic Cytoplasmic Antibody Associated Vasculitis. Indian J Nephrol. doi: 10.25259/IJN_794_2024
Dear Editor,
A 57-year-old female with a history of pulmonary tuberculosis presented with persistent constitutional symptoms, including mild fever, anorexia, asthenia, and cough. The initial treatment for viral fever and subsequent antitubercular drugs failed. Two months later, she developed redness and painful swelling of the right ear [Figure 1a], which resolved post treatment [Figure 1b]. Laboratory investigations showed a rapid rise in serum creatinine (1.8 mg/dL to 3.3 mg/dL), active urinary sediments, and urine protein/creatinine ratio of 1.9 over these two months. The serological evaluation revealed elevated 432 IU/L myeloperoxidase (MPO) titers of antineutrophil cytoplasmic antibody (ANCA). The renal biopsy revealed a core of renal cortical tissue and adjoining medulla with four glomeruli: three globally sclerosed and one showing fibrocellular crescent [Figure 1c]. There was moderate tubular atrophy. Renal medulla showed prominent medullary angiitis characterized by interstitial hemorrhage, karyorrhectic debris, and a polymorphonuclear inflammatory infiltrate [Figure 1d]. Medullary angiitis, cellular crescent, and immunofluorescence suggested pauci-immune crescentic glomerulonephritis. The patient was treated with oral steroids (prednisolone 60 mg daily tapered to 5 mg over six months), six bimonthly doses of cyclophosphamide (500 mg), and later daily azathioprine (2 mg/kg initial tapered to 1 mg/kg) for three years. She was in remission for three years (serum creatinine 1.7 mg/dL, nil proteinuria, negative ANCA). Auricular chondritis is a rare feature of relapsing polychondritis.1 Renal medullary angiitis is a rare but significant lesion often overlooked during biopsy examination.2 The presence of surface markers of vasculitis (inflamed pinna), histological entity of crescentic and medullary angiitis, and good outcomes despite poor prognostic markers (delayed diagnosis, MPO-ANCA positivity, fibrocellular crescent, and medullary vasculitis) was noteworthy.
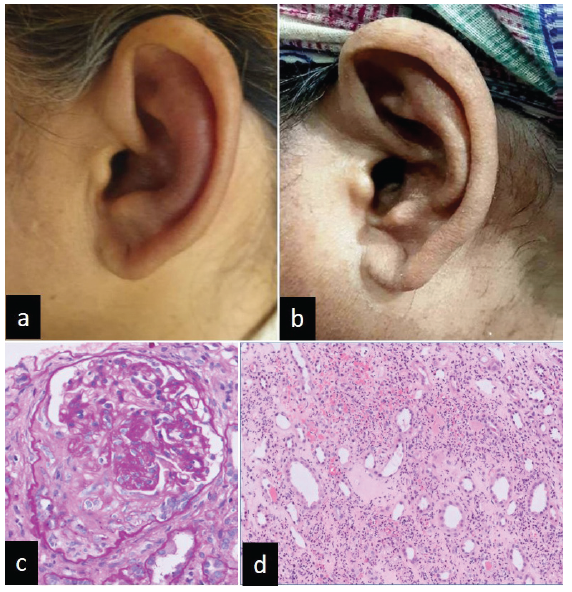
- (a) Left ear inflammation of pinna (b) which resolved (c) photomicrograph showing the single viable glomerulus in the biopsy with the fibrocellular crescent (PAS 400x), (d) photomicrograph depicts the medulla with prominent karyorrhexix, neutrophils, and hemorrhage around the vasa recta (H&E 200x). H&E: Hematoxylin and eosin, PAS: Periodic acid schiff.
Conflicts of interest
There are no conflicts of interest.
References
- Aural manifestations of antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis-diagnosis, symptoms, treatment. J Clin Med. 2024;13:4298.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Renal medullary angiitis: A case series from a single institution. Hum Pathol. 2013;44:521-5.
- [CrossRef] [PubMed] [Google Scholar]




