

Translate this page into:
Blunt Trauma Abdomen Leading to Bilateral Renal Segmental Infarction: Resolving the Enigma
Address for correspondence: Dr. Nidhi Prabhakar, Department of Radiodiagnosis and Imaging, Post Graduate Institute of Medical Education and Research (PGIMER), Chandigarh - 160 012, India. E-mail: nidhirajpalprabhakar@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 38-year-old man was admitted following blunt trauma to chest and abdomen. He underwent computed tomography (CT), which revealed the presence of aberrant renal arteries arising from either side of the abdominal aorta and supplying the lower poles of bilateral kidneys. Posttraumatic thrombosis of the proximal segments of bilateral aberrant renal arteries (for a length of ~4 cm on the right side and ~3 mm on the left side) was seen with resultant segmental infarctions of the lower poles of bilateral kidneys [Figure 1]. Bilateral main renal arteries were normal. Since the patient was hemodynamically stable with adequate urine output and normal renal function tests, the patient was managed conservatively.
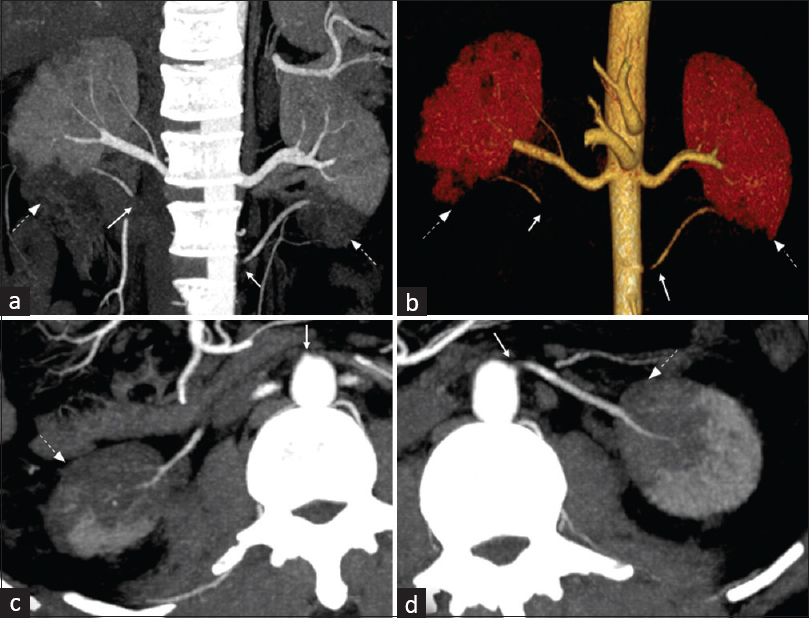
- Images of CECT (Contrast-enhanced Computed Tomography) abdomen in the arterial phase of a 38-year-old-male patient with a history of blunt trauma abdomen showing bilateral aberrant renal artery thrombosis ((white solid arrows) just beyond the aberrant renal arteries’s’ origins from the aorta and segmental infarcts (white dashed arrows) in the lower poles of bilateral kidneys with normal main renal arteries. (a) MIP (Maximun Intensity Projection) coronal curved reformatted image. (b) Volume-rendered image. (c) MIP axial curved reformatted image along the axis of the right aberrant renal artery. (d) MIP axial curved reformatted image along the axis of the left aberrant renal artery
Renal arterial injury is seen in ~0.08% of the cases after blunt trauma abdomen. The mechanism of injury can be stretching of the vessel wall by sudden acceleration–deceleration forces, or it can be due to compression of the vessel wall against the vertebral column after a direct impact. Injury is most common in the proximal part of the artery (within 2–4 cm from its origin). Renal artery injury can be in the form of intimal tears, dissection, thrombosis, pseudoaneurysms, and complete or incomplete transection of the renal artery.[1,2] Segmental or global infarction/necrosis of the kidney, hypertension, and renal failure are a few of the complications of traumatic main or aberrant renal artery thrombosis. Management varies from nonoperative conservative management to endovascular or open surgical repair depending on the hemodynamic stability of the patient, degree of renal infarction, unilateral or bilateral involvement, renal function, presence or absence of active bleeding, and other complications.[3,4]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Endovascular treatment of renal arterial perforation after blunt trauma:Case report. Int J Surg Case Rep. 2018;42:208-11.
- [Google Scholar]
- Traumatic renal artery dissection:From imaging to management. Clin Radiol. 2021;76:153.e17-24.
- [Google Scholar]




