

Translate this page into:
Breaking Barriers: The Case for Inclusive Leadership in Medicine

Corresponding author: Urmila Anandh, Department of Nephrology, Amrita Institute of Medical Sciences and Research Centre, Faridabad, Delhi NCR, India. E-mail: uanandh@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Anandh U, Meena P, Jha V. Breaking Barriers: The Case for Inclusive Leadership in Medicine. Indian J Nephrol. 2025;35:3-7. doi: 10.25259/IJN_420_2024
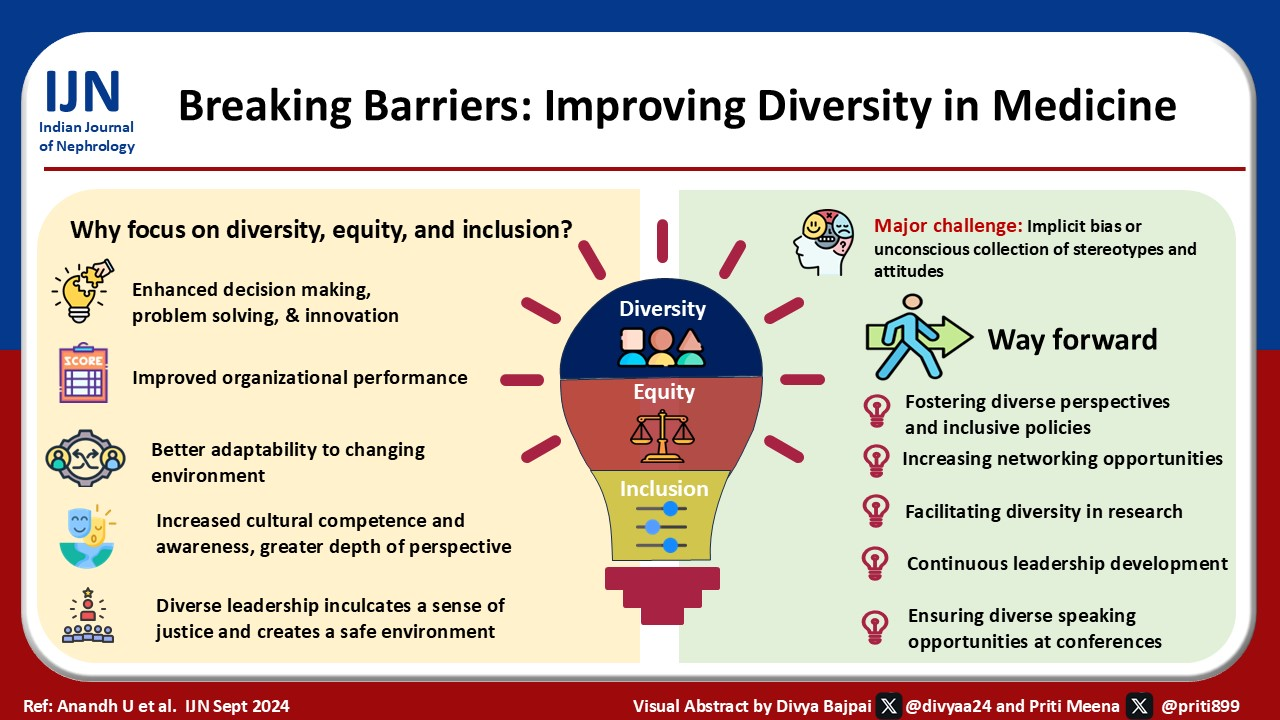
The importance of diversity, equity, and inclusion (DEI) in improving organizational efficiency has gained recognition in recent years. DEI initiatives are being recognized as social and ethical imperatives and strategic necessities to drive innovation, enhance decision-making, and improve overall organizational performance. Organizations with diverse leadership are better equipped to respond to challenges, attract and retain top talent, and meet the needs of diverse populations. The involvement of people of different genders, cultures, social groups, and ability status in all aspects of medical care contributes significantly to the overall improvement in context and resource-sensitive healthcare delivery. Physician diversity has an association with healthcare outcomes.1 Especially; women physicians add value and often make a significant difference in patient outcomes. In a recent study, it was shown that both male and female patients had a lower mortality rate when treated by female physicians. The impact was greater when female physicians took care of female patients than male physicians (adjusted mortality rates: male vs female physicians, 8.15% vs 8.38%; average marginal effect −0.24, CI, −0.41 to −0.07 pp).2
This review explores the current state of DEI in medical leadership, with a focus on professional societies in India, the benefits of increasing DEI, and successful global initiatives that can serve as models for India. While we intend to cover diversity in all dimensions, we use gender diversity as an example to illustrate the general points.
Focus on Diversity
In the Western world context, the DEI conversation is framed around race, ethnicity, gender preferences, and ability status. In India, where the society is also divided by geography, religions, castes, indigenous (tribal) and nonindigenous people, social classes, and other social hierarchies, the situation is far more complex. Historically, individuals have harbored long-held beliefs, attitudes, and behaviors toward those belonging to other groups based on characteristics such as race, gender, age, religion, or social group. There have been many reports of discrimination based on social divisions in academia and medicine in India.3
In recent years, the representation of women in academic medicine has steadily improved, and medical colleges are seeing a greater number of women students. The number of female students joining medical schools in the USA in 2018 was more than that of men (52%).4 According to an analysis of students appearing for the National eligibility Cum Entrance Test (NEET) examination between 2016 and 2019, female candidates outnumbered males by 25%.5 In some colleges, over 60% of the enrolled students are females. Interestingly, specialty preferences show distinct gender differences.6,7 Despite reservations as a form of affirmative action directed toward ensuring appropriate representation of historically disadvantaged groups in education, employment, government schemes, and so on, socially disadvantaged groups remain under-represented compared to their proportions in the general population. Socioeconomic background is a powerful driver to access; students from more privileged backgrounds have better access to resources, coaching, and preparatory materials, which enhances their chances of securing admission to medical colleges.
Mere admission to medical school does not guarantee a fruitful and successful medical career. Few women and minority groups break the glass ceiling to become heads of their departments or professional societies, members of the planning committees in their institutions, receive awards, be part of plenaries of conferences, and join editorial boards of high-impact journals.8,9 For instance, the American Society of Nephrology (ASN) was formed in 1966 by 17 men, and they elected its first women president 43 years later.10 Till now, they have had five women presidents, including the incumbent. The situation has improved in recent years, as the current President is a lady of color and the third consecutive woman to be appointed in this position. The International Society of Nephrology was formed in 1960; its first female President was appointed in 1972, and the second was elected 33 years later. Despite its international nature, 89% of the Presidents have come from North America, Western Europe, and Australia. The European Renal Association, formed in 1963, had its first lady President this year.10 The African Association of Nephrology (AFRAN) has had a single lady President since its inception. The Indian Society of Nephrology has had four female presidents in 55 years of its existence. There has been a single women director out of 16 in the All India Institute of Medical Sciences (AIIMS), New Delhi, and zero out of 13 at the Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh – the two most prestigious public sector medical training institutions in the country. Among the executive directors of the 18 new AIIMS, only 3 are females.11 A snapshot of the gender distribution of the executive committees of various professional bodies and their respective journals in India and the gender composition of various committees of the Indian Society of Nephrology is given in Tables 1 and 2.
| Current President | President elect | Past president | Vice president | Secretary | Joint Sec | Treasurer | EC members (n) M: F | EIC | |
|---|---|---|---|---|---|---|---|---|---|
| Association of Physicians of India | M | M | M | M | M | M | M | 16:2 | M |
| Indian Society of Nephrology | M | M | M | M | M | - | M | 2:0 | M |
| Cardiology Society of India | M | M | M | 4M | M | M | M | 17:0 | M |
| Neurological Society of India | M | M | M | - | M | - | M | 10 : 1 | M |
|
Indian Academy of Neurology (Combined Neurology and Neurosurgery) |
M | F | M | M | M | M | M | 1:3 | F |
| Indian society of Hematology and Blood Transfusion | M | F | F | M | M | M | - | 6:0 | F |
| Endocrine Society of India | M | M | M | M | M | M | M | 6:3 | M |
| Association of Medical Oncologists of India | M | - | - | F | M | M | M | - | - |
| Indian Society of Gastroenterology | M | M | M | - | M | - | M | 6:0 | M |
| Indian Society of Critical Care Medicine | M | F | M | 2:2 | M | M | M | 14:2 | M |
| Indian Chest Society | M | - | M | M | M | M | M | 8:2 | M |
Data as available from the respective society’s website. EIC: Editor in Chief of the official journals of affiliated societies, EC: Executive council members
| Committee | Males | Females |
|---|---|---|
| Constitutional amendment committee | 4 | 1 |
| Liaison committee | 5 | 1 |
| Medicolegal cell | 4 | - |
| Patient advocacy committee | 2 | 3 |
| Social media committee | 7 | 4 |
| Youth committee | 8 | 4 |
| Credentials committee | 5 | 1 |
| Scientific committee | 8 | 2 |
| Zonal members | 4 | 0 |
| Total | 47 | 16 |
Data from websites of various societies.
We do not have high-quality data on the representation of other minority and disadvantaged groups in leadership positions in academic institutions and professional medical societies in India. Out of 1,316,268 students who appeared for the NEET 2024, approximately 11.16% were from scheduled castes, and 4.3% belonged to scheduled tribes.12 Representation of women in medical specialties (other than obstetrics and gynecology) is relatively low. In recent years, there has been an increasing trend in the number of females in specialties such as pediatrics, preventive and social medicine, psychiatry, and dermatology.13
The Association of Surgeons in India has approximately 32,000 members, of which 4160 (12.5%) are women. In a recent survey of female surgeons, most found satisfaction in their choice of profession. However, they face challenges in the form of imposter syndrome and judgmental attitudes of their male colleagues and superiors.14
The Importance of DEI in Leadership
Organizational leadership needs to be diverse to develop and nurture a diverse workforce. The more the leaders are different in their social backgrounds, career stages, lifestyles, choices, and upbringing, the more different opinions are brought to the table. A diverse leadership inculcates a sense of justice and encourages creativity and innovation among members. It creates a safe environment where diverse opinions are considered and valued irrespective of their backgrounds and allows leaders to relate with their base and stakeholders. Many business houses, sports organizations, and media houses realize that the more diverse the leadership, the more effective, varied, and socioculturally appropriate the decisions.
The benefits of diversity in professional society leadership are multifaceted and contribute to organizations’ effectiveness and success in several ways.
Greater depth and breadth of experience and perspective: Diverse leadership teams bring a wide range of experiences and perspectives, which enhance the organization’s ability to relate to different groups and stakeholders. This diversity fosters innovation and increases appeal to a broader audience.
Enhanced decision-making, problem-solving, and innovation: Teams with varied backgrounds and experiences are better equipped to tackle complex problems through more comprehensive and creative decision-making processes. This leads to effective and innovative solutions, problem-solving capabilities, and better organizational decisions and outcomes. The varied perspectives and experiences of a diverse leadership team challenge conventional thinking and encourage new ideas and approaches, thereby fueling innovation.
Increased awareness and cultural competence: Leaders from diverse backgrounds contribute to a greater awareness of the cultural and social dynamics that affect the organizations they lead. This awareness helps them better understand areas where they can exercise influence, enhancing the organization’s reach and impact.
Improved organizational performance: Organizations with diverse workforces tend to have higher productivity, innovation, and member satisfaction levels. A study found that organizations with a diverse workforce have better performance metrics, including increased creativity and problem-solving capabilities.15 Merck Healthcare (in the top quartile for gender diversity) had a 48% higher operating margin and 42% higher returns on sales. Their share earnings were also 45% higher, and the gender-diverse board made better business decisions most of the time.16
Improved relationships with members: Diversity in leadership helps build trust and better relationships with society members. By reflecting the diversity of the community and member base, societies and organizations can better meet and serve the needs and expectations of a wider audience.
Authentic representation, inclusion, retention, and equity: A diverse leadership team helps create an environment that values and practices inclusivity, which is crucial for attracting and retaining top talent to the member base and leadership positions. It helps avoid tokenism by ensuring that diversity is not symbolic but integrated into the core functions and values of the organization. Members feel valued and represented, which enhances their loyalty and commitment. Better representation allows the voices of all stakeholder groups to be brought to the high table to receive appropriate attention.
Adaptability to changing environments: Diverse leadership teams are better equipped to adapt to changing conditions and the needs of various stakeholders. Their varied perspectives help anticipate shifts and adjust strategies accordingly to remain relevant.
The benefits of diversity in networking
The opportunity to meet people of different age groups, genders, and ethnicities, develop relationships, and exchange knowledge, experience, and expertise is critical to professional development. Networking is not only beneficial for the career growth of the individual but also adds value to institutions, organizations, and professional bodies. All individuals, including those from the dominant sociocultural groups, broaden their outlooks by interacting with colleagues from diverse backgrounds. Such networking helps breaks silos and has been crucial to the development of global health initiatives.
Networking opportunities lead to new research and academic collaborations and offer mentorship and leadership guidance. In most situations, individuals with certain behavioral characteristics and traits (extroverts, self-assured) that promote networking come from the dominant sociocultural groups. In contrast, those from different genders and social and ethnic backgrounds may not be able to participate equally vigorously, resulting in lopsided interactions. Networking with “men only” or “dominant social group only” members, the so-called “old boys’ club” still exists. When women try to develop groups that encourage them to socialize among themselves, it is considered feminist.17 These networks determine representation in leadership positions by selectively preferring candidates belonging to an in-group. Improved access to networking opportunities does not happen spontaneously, and steps must be taken to help disadvantaged individuals and groups who do not have prior network models so that they have equitable access to role models and mentors who can help them navigate their journey through all stages of their careers.
Implicit bias and its impact on diversity
Our intent is not to suggest that the lack of diversity is always intentional. Often, it is a result of implicit bias or the unconscious collection of stereotypes and attitudes that individuals develop toward groups of people other than those representing their “in-group.” In professional societies, the excluded groups may include women, minorities, and those from specific geographies or belonging to social groups or institutions different from the dominant group. These biases can influence individual and group behaviors, decisions, and interactions without conscious awareness.
Biases influence networking opportunities and collaboration. Individuals gravitate toward those who share similar backgrounds or characteristics, inadvertently excluding others. This can hinder cross-disciplinary collaboration and limit the exchange of ideas.
Implicit biases impact how professional societies address ethics, diversity, and inclusion issues. Awareness and acknowledgment of bias may help efforts to create equitable and respectful environments.
Mitigating bias
Addressing and mitigating bias requires a proactive and committed approach. It starts with recognizing and acknowledging the problem through self-reflection and developing and implementing a strategy to improve cultural competence and promote inclusivity and diverse perspectives. Other helpful strategies include training programs, goal-setting, monitoring the decision-making process through objective criteria, and holding leaders accountable. Creating safe spaces where individuals feel free to speak up and challenge stereotypes is critical.
Speaking opportunities at conferences
Special mention needs to be made of representation in conferences and panels. Conferences and meetings are platforms for networking and increasing visibility. Despite having similar qualifications and experience, those belonging to the underrepresented groups tend to lose out. Women (and other social groups) are often not considered for speakers or panelist roles. All-male panels (manels) continue to be a reality. One reason is that conference planning and organizing committees have skewed gender representation.
Including speakers from underrepresented groups provides examples of role models and encouragement and mentorship opportunities to younger colleagues from those groups. The presence of women chairs and speakers works as catalysts for the younger female physicians, emboldening them to come forward, interact, and network, thus gaining visibility and confidence. In a study on endocrinology (a specialty where there are 43% women registrars) conferences, only 7% of the questions came from women delegates, and half were queries from women chairs. Male attendees took more time than women (median: 21 vs 15 s) for their questions. Only 9% of the questions were from women in sessions chaired by men. On the other hand, in sessions where all speakers and chairs were women, 57% of all questions were from women. If the first question is by a man, women seem to withdraw, and only 9% of the following question are by women. If a woman delegate starts the Q and A session, 50% of the second question are by women. This study shows that it is not the science but the conference atmosphere that women find intimidating.18 One way to address this inequity and improve gender diversity is to make more women leaders part of conference planning committees. Though this may not make a significant difference, it can be the first step way forward.19
Recognition at the workplace and in meetings is an important benchmark for academic promotions. Removing representational disparities will improve promotional opportunities for the disadvantaged and enable them to reach leadership positions.
Diversity in research
We must point out the gross underrepresentation of certain sections of the population in clinical trials, which causes problems with the generalization of results. Ironically, those with the most pressing health challenges often cannot benefit from these research innovations. A study conducted by the National Academies in the US showed that improving inclusivity and diversity in clinical trials will improve life expectancy (by one year), disability-free life years (by over a year), and increase involvement in the workforce (by 6 months) in women and individuals of racial and ethnic minorities afflicted with type 2 diabetes. An economic analysis revealed that even if 1% of health disparities are alleviated by better inclusion in research, the United States will save $ 40 billion every year as far as diabetes is concerned and another $ 140 billion for heart disease.20 Such data are not available for India.
In conclusion, achieving DEI in medical leadership is a moral and ethical imperative and a strategic necessity that enhances organizational performance, innovation, and patient outcomes. The current state of DEI in medical leadership, particularly in India, reveals significant gaps and challenges, including gender disparities, power imbalance, and implicit biases. Addressing these issues requires a multifaceted approach that includes policy reforms, continuous leadership development, and the creation of inclusive environments that value diverse perspectives. By fostering a culture of inclusivity and actively promoting diversity, medical societies can better reflect the communities they serve, improve healthcare delivery, and drive meaningful social changes. The benefits of such efforts are manifold, ranging from improved personal satisfaction and growth to enhanced organizational resilience and innovation. As we move forward, medical professional societies must commit to sustained DEI initiatives, ensuring that diversity is not just a goal but a fundamental aspect of their operational ethos.
Conflicts of interest
There are no conflicts of interest.
References
- Physician supply, physician diversity, and outcomes of primary health care for older persons in the United States. Health Place. 2004;10:231-44.
- [Google Scholar]
- Comparison of hospital mortality and readmission rates by physician and patient sex. Ann Intern Med. 2024;177:598-608.
- [Google Scholar]
- Casteism among Indian doctors: A critical review. World Journal of Public Health. 2020;5:99-104. Available from: https://doi.org/10.11648/j.wjph.20200504.14
- [Google Scholar]
- AAMC Data. U.S. Medical School Faculty, 2018. Table A-7: Applicants, first -time applicants, acceptees, and matriculants to U.S. medical schools by sex, 2009–2010 through 2018–2019. Available from: http://www.aamc.org
- Available from: https://www.pewresearch.org/decoded/2021/06/ 29/measuring-caste-in-india/ [last accessed on 15 Jul 2024].
- Gender gap in engineering and medical Colleges in India. J Res Sci Math Tech Edu. 2021;4:225-37. Available from: https://doi.org/10.31756/jrmste.434
- [Google Scholar]
- Factors influencing the career preferences of medical students and interns: A cross-sectional, questionnaire-based survey from India. J Educ Eval Health Prof. 2019;16:12.
- [Google Scholar]
- Trends in the proportion of female speakers at medical conferences in the United States and in Canada, 2007 to 2017. JAMA Netw Open. 2019;2:e192103.
- [Google Scholar]
- Women physicians are underrepresented in recognition awards from the association of academic physiatrists. Am J Phys Med Rehabil. 2018;97:34-40.
- [Google Scholar]
- Addressing leadership competency gaps and gender disparities in India’s medical workforce: A call to action. Lancet Reg Health Southeast Asia. 2023;16:100247.
- [Google Scholar]
- Available from: https://medicine.careers360.com/articles/how-many-students-appeared-for-neet [last accessed on 15 Jul 2024].
- Women in modern medicine in India: progression, contribution, challenges and empowerment. Australasian Account Bus Fin J. 2019;13:88-106. https://doi.org/10.14453/aabfj.v13i2.6
- [Google Scholar]
- Realities and challenges for female surgeons: An Indian perspective. IOSR J Dental Med Sci. 2023;5:51-6. https://doi.org/10.1016j.eclinm.2022.10338
- [Google Scholar]
- Available from: https://www.mckinsey.com/featured-insights/diversity-and-inclusion/diversity-matters-even-more-the-case-for-holistic-impact [last accessed on 15 Jul 2024].
- Networking practices and gender inequities in academic medicine: Women’s and men’s perspectives. EClinicalMedicine. 2022;45:101338.
- [Google Scholar]
- Scientific medical conferences can be easily modified to improve female inclusion: A prospective study. Lancet Diabetes Endocrinol. 2021;9:556-9.
- [Google Scholar]
- Are women proportionately represented as speakers at orthopaedic surgery annual meetings? A cross-sectional analysis. Clin Orthop Relat Res. 2020;478:2729-40.
- [Google Scholar]
- Available from: https://nap.nationalacademies.org/resource/26479/Econ_analysis_Infographic.pdf [last accessed on 15 Jul 2024].




