

Translate this page into:
Congenital mesoblastic nephroma: A rare cause of recurrent hematuria beyond infancy
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Congenital mesoblastic nephroma (CMN) tumor is most common benign renal neoplasm in neonates and infants less than 3 months of age, and overall comprises about 3-10% of all childhood renal tumors.[1] Mesoblastic nephroma may be detected on routine prenatal ultrasonography (USG) as early as 26 weeks or may present as a palpable abdominal mass in young infant but presentation beyond infancy that too as gross hematuria is very rare.[2]
A 14-month-old boy, a product of non-consanguineous marriage, presented with complaints of two episodes of painless gross hematuria since 3 months. Urine was red colored throughout the stream with no diurnal variation. There was no history of fever, increased frequency of urine, sore throat, pyoderma, swelling of body or abdomen or periorbital puffiness, skin rash, or drug intake. No antenatal USG was available. On examination, there was pallor; weight was 10.5 kg and height was 79 cm; blood pressure (BP) was 88/54 mmHg; other anthropometric and systemic examinations were unremarkable. Routine and microscopic examination of urine revealed full of red blood cells of normal shape and size in all the fields. Serum calcium was 9.5 mg/dl (N=9.0-11.0 mg/dl), phosphorus 4.5 mg/dl, and alkaline phosphatase 102 U/l. All other tests were within normal limits.
A 5.6 cm × 3.9 cm size hypoechoeic mass lesion with internal echoes identified at the upper pole of right kidney in USG of abdomen. Contrast enhanced computed tomography (CECT) of abdomen revealed reniform, hypodense lesion at the upper pole of right kidney with mild contrast enhancement in the periphery of lesion with foci of dense calcification inferiorly [Figure 1]. Radical nephrectomy was done and excised specimen sent for histopathological examination which was consistent with mesoblastic nephroma of classic type.
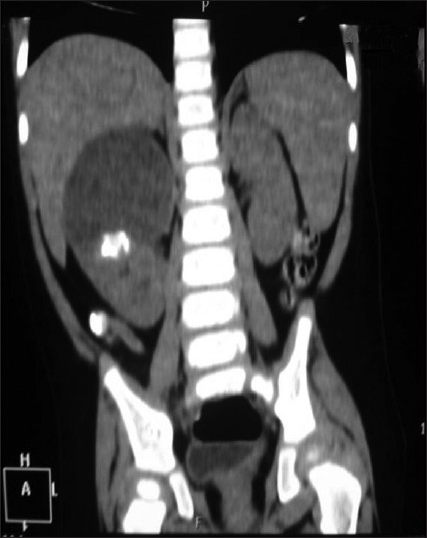
- CECT abdomen showing hypodense mass at the upper pole of right kidney avenging the inferior surface of liver with foci of dense calcification and contrast enhancement in the periphery of lesion
This case is atypical as recurrent gross hematuria at 14 months of age was the presenting feature as there was no intra-abdominal palpable mass. Although hematuria can be associated with CMN (<10% cases), it is not a presenting feature which brings tumor in knowledge. A very few case report say about gross hematuria as presenting feature in CMN.[3]
On imaging, findings suggestive of the classic type include a concentric hyperechoeic and hypoechoeic ring patterns surrounding the tumor in USG. Classic CMN characteristically appears as a large, uniform, soft tissue mass with minimal predominant peripheral enhancement.[4] In comparison; tumors with multiple cystic mass and foci of hemorrhage are much more likely to be consistent with cellular CMN on histology.[5] Nephrectomy alone is usually a sufficient treatment and chemotherapy is not routinely justified. Complete surgical resection remains the most important prognostic factor.[25] Only 5% of the patients have recurrence; therefore, during the 1st year after the nephrectomy, the patient must be submitted to a series of ultrasonographic assessments to detect early signs of local recurrence. There is a long-term low risk of hypertension and proteinuria due to single functioning kidney status that would require annual check-up for BP and urinalysis for proteinuria.[125]
References
- Mesoblastic nephroma: A report of the United Kingdom Children's Cancer and Leukaemia Group (CCLG) Pediatr Blood Cancer. 2011;56:744-8.
- [Google Scholar]
- Congenital mesoblastic nephroma presenting with massive hematuria and hemorrhagic shock: Report of one case. Acta Paediatr Taiwan. 2006;47:135-8.
- [Google Scholar]
- The vascular “ring” sign in mesoblastic nephroma: Report of two cases. Pediatr Radiol. 2003;33:123-8.
- [Google Scholar]
- Imaging of congenital mesoblastic nephroma with pathological correlation. Pediatr Radiol. 2009;39:1080-6.
- [Google Scholar]




