

Translate this page into:
Disseminated Adenovirus Infection in Renal Transplant Recipients
 , Saravanan Margabandhu1,, Elankumaran Krishnan3, Kulaseharan Venugopal Haribabu3, Ram Gopalakrishnan2, Sheba Jacob4, Praveen Balaguru2
, Saravanan Margabandhu1,, Elankumaran Krishnan3, Kulaseharan Venugopal Haribabu3, Ram Gopalakrishnan2, Sheba Jacob4, Praveen Balaguru2
Corresponding author: Saravanan Margabandhu, Department of Nephrology, Apollo Hospitals, Greams Lane, Chennai, Tamil Nadu, India. E-mail: saravananm.dr@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sunder K, Navya M, Athavale J, Margabandhu S, Krishnan E, Venugopal Haribabu K, et al. Disseminated Adenovirus Infection in Renal Transplant Recipients. Indian J Nephrol. doi: 10.25259/IJN_67_2025
Abstract
Adenoviruses rarely cause graft dysfunction in renal transplants and are generally overlooked. We describe two recipients with fever who were diagnosed with disseminated adenovirus infection that resolved with immunosuppression reduction.
Keywords
Adenovirus
Disseminated
Kidney
Renal
Transplant

Introduction
Adenoviruses are dsDNA viruses. Transmission occurs via respiratory droplets or the fecal-oral route, establishing lifelong asymptomatic infections in the lymphoepithelial tissues, renal parenchyma, tonsils, and gastrointestinal tract.1
Case Series
Case 1
A 52-year-old female presented with fever, cough, and abdominal pain 70 days after a deceased donor renal transplant. She was on prednisolone, mycophenolate mofetil, cyclosporine, and valganciclovir. Systemic examination, vitals, complete blood count, and renal function were normal. An ultrasound revealed a 40 cc collection near the lower pole of the transplanted kidney. Ultrasound-guided aspiration was done, and the culture showed no growth. A CT chest revealed patchy ground glass opacities in the right middle lobe. Plasma cytomegalovirus (CMV) quantitative PCR was negative. Blood was sent for adenovirus, CMV, and Epstein-Barr virus (EBV) DNA quantitative PCR. The viral load of the detected adenovirus was 440,189 copies/mL. Disseminated adenoviral infection was diagnosed. Immunosuppression was reduced, following which the fever settled. Viremia decreased to 8,513 copies/mL after 1 month.
Case 2
A 63-year-old male with diabetic nephropathy and decompensated liver disease, on hemodialysis, (NASH-related) underwent a deceased donor combined liver-kidney transplant. His creatinine on discharge was 0.7 mg/dL. Post-op day 23, he was readmitted with fever, cough, and abdominal pain. Vital signs were normal, and physical examination indicated tenderness at the transplant site. COVID and influenza nasopharyngeal swabs were negative. Liver function tests were normal, and serum creatinine increased to 1.5 mg/dL. Blood was negative for CMV and BK virus PCR. Ultrasound and Doppler of both transplanted organs were normal. A PET scan revealed multiple fludeoxyglucose avid hypodense lesions in the transplanted kidney. Ultrasound-guided aspiration was attempted, but the ultrasound showed no liquefaction. Nasopharyngeal swab for multiplex respiratory viral panel detected adenoviruses. Adenovirus quantitative PCR detected 100,091 copies/mL of adenovirus. A graft kidney biopsy revealed scattered PAS-positive intranuclear inclusions in tubules [Figure 1]. Disseminated adenovirus was diagnosed and immunosuppression was reduced. The fever settled in three days, and creatinine reduced to 0.9 mg/dL. Repeat blood testing confirmed undetectable plasma adenovirus load. The patient was asymptomatic with normal renal functions on follow-ups.
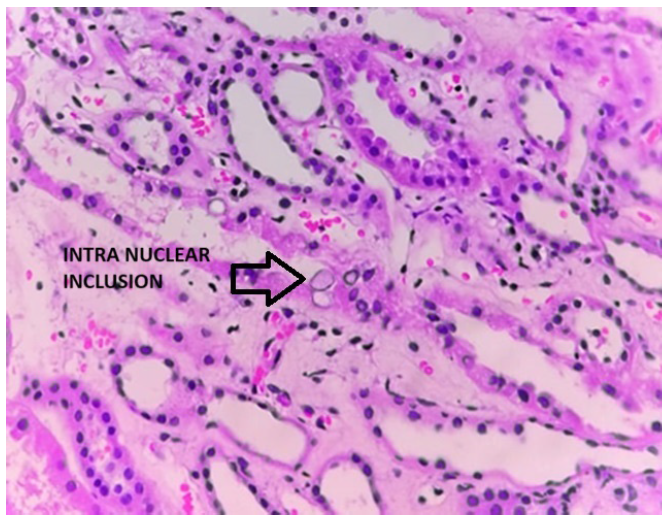
- Adenovirus inclusion bodies. Hematoxylin and eosin stain 40x.
Discussion
Adenoviral infection post-transplant can be donor-derived or due to reactivation of a latent infection acquired before.2 Age of recipient being <5 years, receiving anti-lymphocyte antibodies, and donor-positive/recipient-negative [D+/R-] adenovirus serostatus are risk factors.2,3
Invasive disease occurs in around 10% of patients, and nephritis the most common presentation.2 Hierholzer (1992) estimated that adenovirus infection had 18% mortality risk in renal transplant. Adenovirus can also present as a mass lesion.4 PCR in blood and histopathology are diagnostic. Early hisotpathological changes include eosinohphilic intranuclear inclusions and later stages show basophilic intranuclear inclusions.5 Distal tubules are the most common infection site in the kidney.6 Adenovirus is rarely a space-occupying lesion due to its intense necrotizing nature.6 Reduction of immunosuppression, particularly the antimetabolite, is the mainstay of management. Antiviral options are cidofovir, ribavirin, ganciclovir, brincidofovir, and intravenous immunoglobulin,2 which have all shown varying degrees of success but are rarely used due to their respective toxicities.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
References
- Mandell, Douglas, and Bennett’s principles and practice of infectious diseases - electronic (9th edn). Elsevier - OHCE; 2019. p. :2021.
- Adenovirus infection and transplantation. Transplantation. 2022;106:920-7.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Respiratory viruses: Influenza, RSV, and adenovirus in kidney transplantation. Semin Nephrol. 2016;36:417-2.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Adenoviruses in the immunocompromised host. Clin Microbiol Rev. 1992;5:262-74.
- [CrossRef] [PubMed] [Google Scholar]
- The pathologic spectrum of adenovirus nephritis in the kidney allograft. Kidney Int. 2023;103:378-90.
- [CrossRef] [PubMed] [Google Scholar]
- AJKD atlas of renal pathology: Adenovirus infection. Am J Kidney Dis. 2018;71:e1-2.
- [CrossRef] [PubMed] [Google Scholar]




