

Translate this page into:
Effect of Dialyzer Reuse on the Activity of Paraoxonase 1 in Patients on Hemodialysis
Address for correspondence: Dr. Reynaldo Miguita Jr, Clínica dos Rins Nefronor, Rua Nossa Senhora do Rocio, 154, Cornélio Procópio, Paraná, CEP86300-000, Brazil. E-mail: miguitajunior@gmail.com
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Cardiovascular disease is the major cause of mortality in patients undergoing chronic hemodialysis treatment. The oxidative modification of low-density lipoprotein is a crucial step in the pathogenesis of atherosclerosis. Paraoxonase 1 (PON1) is the protein responsible for most of the antioxidant activity of high-density lipoprotein, and its reduced levels are associated with more cardiovascular events in several populations. In hemodialysis patients, reduced PON1 activity has been shown to be associated with increased cardiovascular mortality. Studies have shown that after the hemodialysis session, the activity of PON1 increases. The influence of dialyzer reuse on the activity of PON1 is unknown. We aimed to evaluate the effect of the reuse of two types of dialyzers (polynephron and polyethersulfone) on the PON1 activity of hemodialysis patients.
Subjects and Methods:
A total of 30 patients on hemodialysis were included. Pre- and post-dialysis blood samples were collected to analyze the activity of PON1 in thefirst use of the dialyzer and in the hemodialysis session of its sixth reuse. This process was carried out with polynephron (bisphenol-free) and polyethersulfone dialyzers.
Results:
We found that post-dialysis PON1 activity was significantly higher than pre-dialysis activity in both thefirst use and sixth reuse (P < 0.001).
Conclusion:
The practice of reusing the dialyzer did not interfere with the improvement of PON1 activity after the hemodialysis session.
Keywords
Cardiovascular diseases
chronic kidney disease
hemodialysis
oxidative stress
paraoxonase 1

Introduction
Cardiovascular diseases (CVDs) are the leading cause of death in end-stage renal disease (ESRD) patients. They have a multifactorial genesis and account for almost 50% of deaths in this population.[12] Patients on hemodialysis have an abnormal lipid profile characterized by elevated levels of triglycerides and low-density lipoproteins (LDL) and decreased levels of high-density lipoprotein (HDL).[3]
Paraoxonases are enzymes that were initially described for their ability to hydrolyze exogenous organophosphorus compounds, such as the active metabolite of the agricultural pesticide parathion, paraoxon.[4] Paraoxonase 1 (PON1) has attracted significant interest in being the protein responsible for most of the antioxidant activity of HDL. PON1 associated with HDL acts to prevent the oxidation of LDL and its deleterious effects.[56] Paraoxonase activity is decreased in patients on chronic maintenance hemodialysis.[7] Reduced levels of PON1 activity are associated with increased occurrence of cardiovascular events in several populations.[8910] In hemodialysis patients, reduced PON1 activity has been shown to be associated with increased cardiovascular mortality.[11]
The oxidative modification of LDL is a crucial step in the pathogenesis of atherosclerosis.[12] Plasma lipid oxidation by peroxynitrite is increased in patients with ESRD, and this effect is worsened by hemodialysis.[13]
The dialyzer membranes are made of different substances such as cellulose, modified cellulose, synthetic cellulose, and synthetic membranes such as polyethersulfone, which are more biocompatible. Recently, a new synthetic membrane, polynephron, has been introduced in the market. Such a membrane is composed of polyethersulfone, but unlike other dialysis membranes, it does not contain bisphenol (BPA), an agent with the potential to interfere with the functioning of various endocrine glands, in its structure. A study has shown a significant increase in plasma BPA in patients who are hemodialyzed with polyethersulfone membranes, and that the reverse occurs in dialyzed patients with polynephron. In addition, there was an increase in oxidative stress markers in patients using polyethersulfone compared to polynephron.[14]
Dialyzer reuse is still a subject of many controversies. With the advent of modern, more biocompatible membranes and more favorable sterilization techniques, there is no compelling medical indication for reprocessing dialyzers. The inherent risks of the reuse process exist, even with the application of all requirements from the Association for the Advancement of Medical Instrumentation (AAMI).[15] The practice of reusing the dialyzer persists in countries where the economic factor is a barrier to the practice of single use. Most low-income countries employ reuse in almost 100% patients in renal replacement therapy.[16]
Studies have shown that after the hemodialysis session, the activity of PON1 increases.[1718] The influence of the reuse and the dialyzer membrane type on the activity of PON1 is unknown. Patients on hemodialysis have increased oxidative stress and inflammation that are associated with elevated cardiovascular mortality.[19] The purpose of our study was to evaluate the effect of the reuse of two types of dialyzers on the activity of PON1 in hemodialysis patients.
Subjects and Methods
Patients and research design
This is a quasi-experimental study which included ESRD patients on hemodialysis at the Instituto do Rim de Londrina – Histocom. The study inclusion criteria were age >18 years, being from thefirst shift of hemodialysis (from 6:00 a.m. to 10:00 a.m.), and on hemodialysis treatment for at least 3 months. Patients could not participate if they were dialyzing through a central catheter, had a cancer, had an active infection that caused hospitalization in the last 15 days before collection of blood for the study, had serological positivity for hepatitis B, hepatitis C, and human immunodeficiency virus (HIV), had a life expectancy less than 6 months, and had a history of reduced dialyzer reuse. The Local Ethics Committee of Londrina State University approved the study protocol, and the study was performed in accordance with Helsinki Declaration. Written informed consent was obtained from all subjects.
Data collection and laboratory measurements
The period of study was from September to October 2016. Pre- and post-dialysis samples were collected at four moments for the determination of PON1 activity, as described in Figure 1.

- Flow diagram of the study
Characteristics of dialysis treatment and dialyzer reprocessing
All patients were dialyzed thrice weekly for 3½–4 h per session with blood flow rates of 300–400 mL/min and dialysate flow rates of 500 mL/min using bicarbonate buffer. Heparin was used for anticoagulation. The hemodialysis prescriptions were individualized with the goal of single pool Kt/V (sp Kt/V) higher than 1.2. Reprocessing machines using 0.2% peracetic acid as a disinfectant performed reuse of the dialyzers. The analysis of water used for hemodialysis and reprocessing of the dialyzers presented less than 0.25 endotoxin units and zero bacteria, meeting the standards required by Brazilian legislation and the AAMI. The hemodialysis water treatment of the Instituto do Rim de Londrina – Histocom is composed of pretreatment with sand filters, softener, two activated carbon filters, and reverse osmosis system by double pass.
Blood collection was scheduled on the day of routine monthly exams, after an 8-h fasting. Before heparinization and initiation of the hemodialysis session, 10 mL of blood was collected for analysis of PON1 activity. Patients receiving hemodialysis at the Instituto do Rim – Histocom use polynephron dialyzers. A new dialyzer was opened for each patient on the study'sfirst day. At the end of the hemodialysis session, before withdrawal of the fistula needles, another 10 mL of blood was collected for the same analyses that were performed predialysis. At the hemodialysis session of the sixth reuse, blood samples were collected in the same manner for the determination of PON1 activity. Patients continued to use polynephron dialyzers, and after a 2-week interval, in the following month, on the date of the routine monthly exams, polyethersulfone dialyzers were opened and the study protocol was repeated in a way like that already specified for the polynephron dialyzers.
The blood samples were collected in vacuum tubes and stored in a refrigerator for up to 4 h. They were then transported in a refrigerated container (ice cube box) to the Post-Graduation Laboratory of the University Hospital of the Londrina State University within 15 min. Plasma samples were separated from cells by centrifugation at 3000 rpm for 10 min, and the remaining blood was washed three times with 9 g/L NaCl solution. Samples were analyzed either on the same day or stored at −80°C until further analysis.
The total activity of PON1 was determined using the methodology described by Richter et al.[20] Measuring the rate of phenylacetate hydrolysis for the determination of PON1 activity was performed on a Perkin Elmer® microplate reader EnSpire model (Waltham, MA, USA). The total activity of PON1 is expressed in U/mL.
Statistical analyses
Initially, a descriptive analysis of the data was performed. Then, an exploratory analysis was conducted to evaluate normal distribution (Shapiro–Wilk test) and homogeneity of variance (Levene test) of each variable. For the variables that did not confirm to the assumptions of normality, Wilcoxon matched-pairs signed-ranks test was performed, and the data were presented as median and 25th–75th quartiles. When three or more variables were analyzed, Friedman test (nonparametric repeated measures analysis of variance [ANOVA]) was used. For continuous variables with Gaussian distribution, values were expressed as means and standard deviations. A statistical significance of 5% was adopted (P < 0.05). The software Statistical Package for the Social Sciences (SPSS) 11.5 for Windows (SPSS, Inc., Chicago, IL, USA) was used for data analyses.
Results
A total of 30 patients on maintenance hemodialysis for more than 3 months were included in this study. The demographic and laboratory characteristics of the study participants are given in Table 1. The median pre-dialysis PON1 activity in thefirst use of the polynephron dialyzer was 139.4 U/mL and the post-dialysis activity was 181.5 U/mL (P < 0.001). These results were maintained in the dialyzer sixth reuse with a pre-dialysis PON1 activity of 133.5 U/mL and a post-dialysis PON1 activity of 166.7 U/mL (P < 0.001). The PON1 activity improved significantly after the hemodialysis sessions both on thefirst and sixth reuse of the polyethersulfone dialyzer, like the polynephron dialyzer (P < 0.001) [Figure 2]. The reuse of the dialyzer, either polynephron (without BPA) or polyethersulfone, did not influence the degree of post-dialysis increase of PON1 activity.
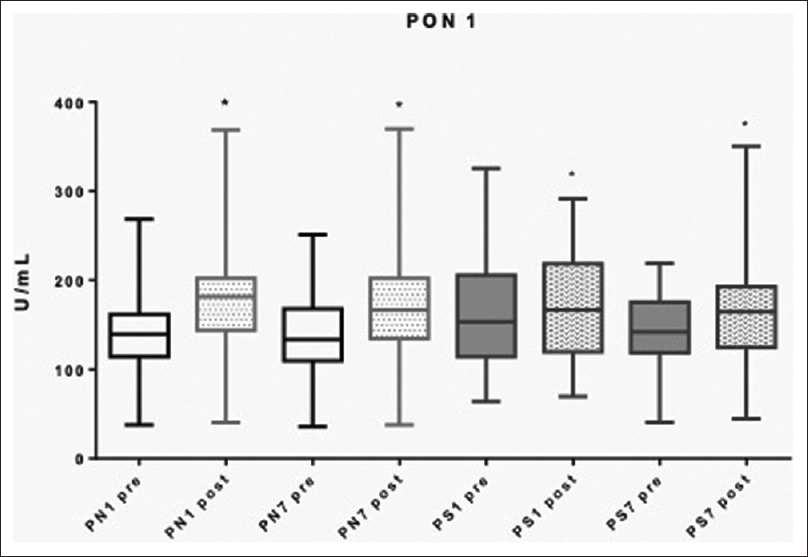
- Median PON1 activity pre- and post-dialysis in PN and PS dialyzers in thefirst (1) and seventh (7) use (sixth reuse). *P < 0.001 compared to the pre-dialysis activity levels. PN = polynephron, PON1 = paraoxonase 1, PS = polyethersulfone
| Age (years, mean±SD) | 52.6±13.7 |
| Male gender, no. (%) | 18 (60) |
| Dialysis vintage (months, mean±SD, median) | 81.26±79.03, 39 |
| Albumin (g/dL, mean±SD) | 4.06±0.40 |
| Co-existing illnesses, no. (%) | |
| Diabetes | 8 (26.6) |
| Hypertension | 26 (86.6) |
| Medications, no. (%) | |
| Statin | 9 (30) |
| Folic acid | 7 (23.3) |
| Erythropoietin | 27 (90) |
SD: Standard deviation
Discussion
The lower activity of PON1 in hemodialysis patients may be due to uremic toxins and increased oxidative stress. Hemodialysis promotes reduction of these uremic toxins, and thus could justify the elevation of PON1 levels after the hemodialysis session. In our study, we found an increase in PON1 activity after hemodialysis sessions, as other researchers have already demonstrated.[1718] The reuse of the dialyzer, either polynephron (without BPA) or polyethersulfone, did not influence this increase. PON1 protects LDL from the oxidative action of reactive oxygen species (ROS), and thus contributes to the athero-protective effect of HDL.[62122] PON1 protects HDL from peroxidation and improves reverse cholesterol transport; furthermore, PON1 degrades bioactive phospholipids, such as platelet-activating factor, which has proinflammatory and prothrombotic properties.[2324] In addition, PON1 promotes the hydrolysis of homocysteine thiolactone and prevents hyperhomocysteinemia, a process involved in atherogenesis.[25] Since reduced levels of PON1 have been associated with increased cardiovascular mortality in hemodialysis patients,[11] strategies that improve PON1 levels or that do not worsen PON1 activity are important. Reusing the dialyzer was safe in the context of PON1 activity because it did not interfere with its post-dialysis improvement. There was no superiority between the membranes studied in relation to PON1 activity.
Only 20% of the people requiring renal replacement therapy are able to get treated in about 100 developing countries, that account for 50% of the world's population.[26] These numbers illustrate the fact that, although reuse practice is less evident in developed countries such as the USA, Japan, and Germany, this practice should remain as a support option for the practice of hemodialysis in developing countries such as India, Brazil, Southeast Asia, South America, and Africa.
So, in summary, our study did find an increase in PON1 activity after the hemodialysis sessions until the sixth reuse of the dialyzers, regardless of the dialyzer membrane tested. This study is rather reassuring in the context that, in the studied conditions, the reuse did not promote worsening in PON1 activity, which could aggravate the oxidative stress in these patients.
Our study has few limitations. For instance, we have just studied two kinds of membranes and our results cannot be extrapolated for more than six reuses of dialyzers. Future studies comparing a larger number of patients initiating hemodialysis with single use of dialyzer versus patients initiating hemodialysis with the practice of reusing the dialyzer could provide more robust elements with respect to PON1 activity in these situations.
We conclude from this study that the practice of reusing the polyethersulfone and polynephron dialyzers (at least for six reuses, and with the described methods) does not interfere with the improvement of PON1 activity after the hemodialysis session.
Statement of ethics
Patients have given their written informed consent, and the study protocol has been approved by the research ethics committee of the Londrina State University.
Author contributions
All the authors participated and contributed to the process of conception and design of the study, collecting data and performing analyses in this study. All the authors contributed by writing and revising the manuscript.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;32((5 Suppl 3)):S112-9.
- [Google Scholar]
- US renal data system 2015 annual data report: Epidemiology of kidney disease in the United States? Am J Kidney Dis. 2016;67((3 Suppl 1)):Svii, S1-305. doi: 10.1053/j.ajkd. 2015.12.014
- [Google Scholar]
- The story of PON1: How an organophosphate-hydrolysing enzyme is becoming a player in cardiovascular medicine. Neth J Med. 2006;64:34-8.
- [Google Scholar]
- Paraoxonase prevents accumulation of lipoperoxides in low-density lipoprotein. FEBS Lett. 1991;286:152-4.
- [Google Scholar]
- Serum paraoxonase activity and protein thiols in chronic renal failure patients. Indian J Nephrol. 2008;18:13-6.
- [Google Scholar]
- Antioxidant and anti-inflammatory role of paraoxonase 1: Implication in arteriosclerosis diseases. N Am J Med Sci. 2012;4:523-32.
- [Google Scholar]
- Low human paraoxonase predicts cardiovascular events in Japanese patients with type 2 diabetes. Acta Diabetol. 2009;46:239-42.
- [Google Scholar]
- Paraoxonase (PON1) and the risk for coronary heart disease and myocardial infarction in a general population of Dutch women. Atherosclerosis. 2008;199:408-14.
- [Google Scholar]
- Human serum paraoxonase concentration predicts cardiovascular mortality in hemodialysis patients. Clin Nephrol. 2007;67:358-65.
- [Google Scholar]
- Peroxynitrite-induced oxidation of plasma lipids is enhanced in stable hemodialysis patients. Kidney Int. 2003;63:2207-13.
- [Google Scholar]
- The choice of hemodialysis membrane affects bisphenol A levels in blood. J Am Soc Nephrol. 2016;27:1566-74.
- [Google Scholar]
- Single-use versus reusable dialyzers: The known unknowns. Clin J Am Soc Nephrol. 2007;2:1079-86.
- [Google Scholar]
- Dialyzer reuse and mortality risk in patients with end-stage renal disease: A systematic review. Am J Nephrol. 2012;35:249-58.
- [Google Scholar]
- Paraoxonase-1 concentrations in end-stage renal disease patients increase after hemodialysis: Correlation with low molecular AGE adduct clearance. Clin Chim Acta. 2007;377:213-20.
- [Google Scholar]
- Serum paraoxonase 1 (PON1) lactonase activity is lower in end-stage renal disease patients than in healthy control subjects and increases after hemodialysis. Clin Chem Lab Med. 2011;49:61-7.
- [Google Scholar]
- Cardiovascular risk in chronic kidney disease. Kidney Int. 2004;66((Suppl 92)):S11-5.
- [Google Scholar]
- Determination of paraoxonase 1 status without the use of toxic organophosphate substrates. Circ Cardiovasc Genet. 2008;1:147-52.
- [Google Scholar]
- Protection of low-density lipoprotein against oxidative modification by high-density lipoprotein associated paraoxonase. Atherosclerosis. 1993;104:129-35.
- [Google Scholar]
- HDL, its enzymes and its potential to influence lipid peroxidation. Atherosclerosis. 1995;115:243-53.
- [Google Scholar]
- Paraoxonase inhibits high-density lipoprotein oxidation and preserves its functions. A possible peroxidative role for paraoxonase. J Clin Invest. 1998;101:1581-90.
- [Google Scholar]
- Hydrolysis of platelet-activating factor by human serum paraoxonase. Biochem J. 2001;354:1-7.
- [Google Scholar]
- Hyperhomocysteinemia, paraoxonase activity and risk of coronary artery disease. Clin Biochem. 2006;39:821-5.
- [Google Scholar]
- The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int. 2011;80:1258-70.
- [Google Scholar]




