

Translate this page into:
Effects of COVID-19 Pandemic on Patients with Kidney Disease and Kidney Replacement Therapy: Focus on Black, Asian, and Minority Ethnic Groups: A Systematic Review
 , Vinay Sankurshetty3, Odunayo Ashimolowo3, Chris Bark4, Abby Kendrick5, Ala Szczepura3, Nithya Krishnan1,3
, Vinay Sankurshetty3, Odunayo Ashimolowo3, Chris Bark4, Abby Kendrick5, Ala Szczepura3, Nithya Krishnan1,3
Corresponding author: Oluwafemi Efuntoye, Renal Services Department, University Hospital Coventry and Warwickshire NHS Trust, Coventry, United Kingdom. E-mail: Ololadephemmy@gmail.com
Ifeoma Faith Agburum, Renal Services Department, University Hospital Coventry and Warwickshire NHS Trust, Coventry, United Kingdom. E-mail: Ifeoma.Agburum@uhcw.nhs.uk
-
Received: ,
Accepted: ,
How to cite this article: Efuntoye O, Agburum IF, Baharani J, Sankurshetty V, Ashimolowo O, Bark C, et al. Effects of COVID-19 Pandemic on Patients with Kidney Disease and Kidney Replacement Therapy: Focus on Black, Asian, and Minority Ethnic Groups: A Systematic Review. Indian J Nephrol. doi: 10.25259/IJN_281_2024
Abstract
Background
COVID-19 pandemic significantly affected health services globally, resulting in poorer outcomes, especially in patients with chronic long-term illnesses. For patients with chronic kidney disease (CKD), potential effects might include, among others, disruption of dialysis services, reduced kidney transplant rates, and increased incidence of severe COVID-19 infections and death. Such differences may be further exacerbated in patients from Black, Asian, and Minority Ethnic (BAME) populations with CKD.
Aim
To conduct a systematic review to identify the global impact of COVID-19 on kidney replacement therapy and to determine the extent of any disparities in BAME patients with CKD.
Materials and Methods
PubMed, Embase (OVID), and CINAHL (EBSCO) databases were searched for relevant studies published between January 1, 2019, and November 24, 2023. Predetermined inclusion/exclusion criteria were utilized to shortlist abstracts. Two reviewers independently appraised articles and systematically extracted data and assessed the quality of studies. Thematic analysis was used for evidence synthesis; no quantitative meta-analysis was conducted. The review was registered with PROSPERO (CRD42020201771).
Results
Two hundred and eleven abstracts were shortlisted, 52 articles were identified for full-text review, and 20 articles published worldwide were included in the final review. Themes identified included: effects of the COVID-19 pandemic on patients with CKD undergoing dialysis (six studies); impact on kidney transplant recipients and transplant programs (eight studies); and differential impact of COVID-19 on BAME patients in comparison with the general population (six studies). The presence of CKD in patients with COVID-19 was identified as a poor prognostic factor, along with obesity, lower socioeconomic status, and BAME population.
Conclusion
The findings of this targeted review demonstrate the global impact of COVID-19 on various aspects of kidney replacement therapy and provide evidence of important disparities for BAME patients. In case of any future pandemic, vulnerable groups undergoing hemodialysis and those with kidney allografts will require special attention and care.
Keywords
COVID-19
Pandemic
BAME
Hemodialysis
Transplantation

Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has resulted in over 500 million confirmed COVID-19 cases and more than six million deaths since December 2019.1 Infection causes a respiratory syndrome with presentation ranging from asymptomatic individuals to SARS in almost 5% of affected subjects; critical cases are characterized by organ failure, including the kidneys and sometimes death.2
The COVID-19 pandemic significantly affected various health services globally, resulting in poorer outcomes, especially in patients with long-term illnesses, including chronic kidney disease (CKD). Dialysis is the mainstay of treatment for patients with advanced kidney disease, including peritoneal dialysis and hemodialysis, which can be delivered home-based or hospital-based. However, kidney transplantation remains the best long-term treatment option to improve survival and quality of life.3 Kidney transplantation can also be lifesaving when vascular access options are lost in patients with advanced kidney disease.4,5 Before the pandemic, at the end of 2019, more than 58,000 European patients were waiting for an organ transplant.6 Annually, 3–4% of these patients would die before being transplanted.6 Worldwide, the impact of COVID-19 on patients with CKD appears to have been wide-ranging, including disruption of dialysis services; a marked reduction in kidney transplant surgeries; and increased susceptibility to severe COVID-19 for those with a poor immune response or those from lower socioeconomic class, more especially the Black, Asian, and Minority Ethnic (BAME) groups.7–9 These groups often face socioeconomic and structural inequalities that often contribute to disparities in health outcome. These disparities can include limited access to healthcare, higher rate of comorbidities, and living in overcrowded environments.10
This review is driven by the pressing need to thoroughly comprehend how the COVID-19 pandemic impacts patients with CKD and kidney replacement services, particularly within vulnerable groups like BAME communities. Such insights are pivotal for crafting tailored interventions and policy measures to mitigate the pandemic’s adverse effects on CKD patients and address healthcare disparities among BAME populations.
This review aimed to identify and assess research evidence of the impact of the COVID-19 pandemic on patients with CKD (incidence, clinical outcomes, hospitalization need, and healthcare disparities) and on kidney replacement services worldwide as well as evidence of any specific impact on BAME populations. The review protocol was submitted for peer review to the International Prospective Register of Systematic Reviews (PROSPERO) ID: CRD42020201771.11 A mixed-methods approach to evidence synthesis was specified in the protocol to allow for inclusion of different study designs, in addition to randomized controlled trials.12 There was strict adherence to international guidelines on Preferred Reporting Items for Systematic review and Meta-Analyses (PRISMA) guidelines.13
Search strategy
Literature searches were undertaken by specialist health librarians (CB and AK) qualified in clinical and systematic reviews and informed by an initial scoping review. The databases searched were PubMed, Embase (OVID), and CINAHL (EBSCO). These were selected as the most likely to report studies focused on the main research question and to ensure that staff time was utilized most efficiently. Tailored search strategies were devised for individual databases [Appendix 1]. Searches covered the period from January 1, 2019, to November 24, 2023.
Study selection
Papers were screened against predetermined inclusion and exclusion criteria, as shown in Table 1. Abstracts were reviewed blind by two readers and shortlisted against these. The study designs included cohort studies, case series, surveys, and cross-sectional studies. All shortlisted articles were imported into the Rayyan database and a separate file was prepared for each database searched. Full articles were downloaded and their content examined independently by two reviewers (blind review). A third reviewer compared final short-lists and any differences were resolved by discussion between the two original reviewers; if arbitration was required, then this was provided by another member of the review team (OE, IA, JB, VS, OA, AS, and NK participated in this process). This process minimized any selection bias. The details of all articles were entered into an Endnote library and bibliographies were scrutinized to identify possible additional studies. The abstract screening and shortlisting data are presented as a PRISMA flow diagram.
| Descriptor | Inclusion criteria | Exclusion criteria |
| Population |
Patients with Chronic Kidney Disease, Renal Dialysis or Kidney Transplant (KD-RD-KT) Dialysis patients (all ages). Renal transplant patients (all ages). To include multi-organ transplants if kidney transplantation is included. COVID-19 patients to include those with clinical indications and positive swab |
Organ transplants without kidney transplant Conservative management for ESRD patients |
| Comparator |
KD-RD-KT service provision in pandemic period. KD-RD-KT service provision for patients from BAME communities |
Ethnicity ‘mentioned in passing’ and not a significant focus |
| Study design |
All qualitative and quantitative studies. To include non-experimental observational pre- and post-2020 (cross-sectional, case-series), surveys/interviews/focus groups, studies exploring perspectives of patients/ doctors (qualitative), reviews. |
Single case reports |
| Impact of COVID-19 (pre-and post-2022). |
Impact on care of KD-RD-KT patients Impact on morbidity and mortality linked to kidney disease complications or post-COVID sequelae. Impact on patients’ hospital outpatient attendances, GP surgery consultations, prescriptions and receiving medication. |
Does not report historical and/or BAME differential impact. |
| Other |
Article in English language All relevant original studies, including conference and abstracts irrespective of country. |
English abstract only Publications in non-peer-reviewed journals/conferences |
ESRD: End-stage renal disease, BAME: Black, Asian and Minority Ethnic, GP: General practitioner
Data extraction and quality assessment
Summary Table [Table 2] collected common information from all articles including author names, publication date and country of publication, study design, aims and objectives, patient population (kidney disease/renal dialysis/renal transplant); sample size and demographics (age, gender, and ethnicity); and outcomes recorded and conclusions.
| Author names/years/country | Study design | Aims and Objectives | Patient population | Sample size | Outcomes and conclusion |
|---|---|---|---|---|---|
| Hsu et al. 2021 USA14 | Cohort | To characterize the risk factors for and outcomes following COVID-19 among patients on hemodialysis. | Dialysis patients | 1,948 | COVID-19 is common among patients receiving maintenance dialysis, particularly those residing in congregate settings. Among maintenance dialysis patients with COVID-19, mortality is high, exceeding 20%. |
| Long et al. 2021 USA33 | None | To highlight the current understanding of the pathophysiology of COVID-19-associated kidney injury and the impact COVID-19 may have on long-term kidney function. | Patient with AKI and CKD | The review emphasizes the unknown long-term effects of COVID-19 on kidney health, stressing the need for prospective studies to assess the incidence of chronic kidney disease post-infection. It also calls attention to genetic and healthcare disparities that may contribute to varying impacts across different population groups. | |
| Khatri et al. 2021 USA19 | Cohort | To determine the sero-prevalence of COVID-19 antibodies in hemodialysis population and its implications for public health. | Dialysis patients | 361 (median age: 68, 45% whites, 34% blacks and 11% Hispanic) | Among 361 patients, 28% tested positive for SARS-CoV-2 antibodies or PCR. Prevalence rates varied by dialysis unit, with significant differences observed. Positive patients were younger and more likely to be of Black or Hispanic ethnicity. High rates of asymptomatic infection, hospitalization, and mortality were noted among end-stage kidney disease patients. |
| Mohan et al. 2021 USA21 | Cohort | To describe 2020 mortality patterns during the COVID-19 pandemic in the United States among kidney transplant candidates and recipients. | Kidney transplant recipients and candidates | 4,114 12% of all COVID-19-related waitlist deaths occurred in Black or Hispanic candidates unlike 15% in white. | In 2020, 11% of waitlisted patient deaths were due to COVID-19, with a higher likelihood observed among males, obese individuals, and those from racial/ethnic minority groups. This study highlights elevated mortality rates linked to COVID-19 among both waitlisted candidates and kidney transplant recipients in the US during 2020. |
| Salerno et al. 2021 USA15 | Cohort | To identify risk factors associated with COVID-19 and mortality in Medicare patients undergoing long-term dialysis. | Dialysis patient | 498, 169 median age, 66 years; 43.1% women and 56.9% men. | Among Medicare patients receiving long-term chronic dialysis, COVID-19 and mortality rates were notably elevated in Black and Hispanic individuals compared to non-Black patients. These findings underscore the importance of recognizing COVID-19 risk factors and outcomes in this population, guiding policy decisions aimed at reducing the disproportionate burden of COVID-19 and mortality. |
| Taaji et al. Canada17 | Cohort | To describe the incidence, risk factors and outcomes for infection in these patients in Ontario, Canada. | Dialysis patients | 12, 501 | Patients undergoing long-term dialysis are at increased risk of SARS-CoV-2 infection and death from coronavirus disease 2019. |
| Schold et al. 2021 USA24 | Cohort | To identify rates and independent risk factors for COVID-19 mortality among kidney transplant candidates in the United States over the first 9 months of the pandemic. | Kidney transplant candidates | 131, 659 | Factors associated with increased COVID-19 mortality included increased age, males, higher body mass index, diabetes and race (Blacks and Hispanics). Among kidney transplant candidates in the United States, social determinants of health in addition to demographic and clinical factors are significantly associated with COVID-19 mortality. |
| Elias et al. 2020 USA20 | Cohort | To evaluate the prevalence of COVID-19 disease in a non-selected population of kidney recipients. To identify the demographics, comorbidities, and clinical and functional parameters associated with COVID-19 disease in this specific population. | Kidney transplant recipients | 1,216 | Kidney transplant recipients were actively followed up during the pandemic in France. Patients with kidney transplants display a high risk of mortality. Non-White ethnicity and comorbidities such as obesity, diabetes, asthma, and chronic pulmonary disease were associated with higher risk of developing COVID-19 disease. |
| Lum et al. 2020 USA23 | Cohort | To evaluate mortality outcomes among kidney transplant recipients at a centre with a high burden of cases but not experiencing acute crisis due to COVID-19. | Kidney transplant recipients | 41 (Hispanic 65.9%, black 14.6%) | The majority of COVID-19 infections affected individuals from minority groups, with 65.9% being Hispanic and 14.6% Black. Kidney transplant recipients experienced heightened severity, leading to increased hospitalization and mortality rates compared to the general population. |
| Tabinor et al. 2021 UK27 | Prospective observational study | To assess whether being from BAME is independently associated with mortality in end-stage kidney disease (ESKD) patients with COVID-19. | Patient with ESRD | 3,379 | During the 8-week observation, 191 individuals were diagnosed with COVID-19, comprising 84% hemodialysis, 5% peritoneal dialysis, and 11% kidney transplant recipients (KTR). BAME ESKD patients with COVID-19 exhibited over twice the likelihood of mortality compared to White patients. |
| Corcillo et al. 2020 UK31 | Cohort | To describe the clinical features and outcomes ESRD patients admitted with COVID-19. | Patients with ESRD | 39 consecutive ESRD patients (28 on HD and 11 with renal transplant) | This report stated the clinical features and outcomes of 39 ESRD patients with diabetes and admitted with COVID-19 infection. The mortality rate was about 36%. There is a high prevalence of patients of Afro-Caribbean ethnicity. |
| Miller et al. 2021 USA22 | Observational study with a retrospective design. | To examined the effects of COVID-19 on solid organ waiting list mortality in the United States and compared effects across patient demographics and donation service areas. | Kidney transplant candidates | They examined the effects of COVID-19 on solid organ waiting list mortality in the United States and compared effects across patient demographics (e.g., race, age, and sex) and donation service areas. The only demographic group with increased waiting list mortality were Blacks versus Whites for kidney candidates. | |
| Crews et al. 2020 USA32 | None | To explain the impact of the COVID-19 pandemic and structural racism on racial disparities in health, particularly among Black Americans. | BAME | The authors highlighted the role of fear and anticipated poor treatment within the BAME community as contributing factors to the disparities in COVID-19 impact compared to white populations, advocating for equitable care provision and the involvement of community leaders to promote trust and educate on the benefits of timely healthcare during global health crises. | |
| Clarke et al. 2022 USA25 | Observational study | To quantify the spatiotemporal trends in excess mortality rates in heart, kidney, liver, and lung SOT recipients in the United States and compare those rates to the overall US population. | Kidney transplant recipients | 52, 028 Heart, 340 711 kidney, 129 412 liver, and 28 687 lung transplant recipients. | The overall conclusion suggests that excess mortality rates are higher in SOT recipients compared to the general population, with variations among different organ groups and racial/ethnic categories. |
| Savino et al. 2021 UK18 | Retrospective cohort | To describe the incidence of COVID-19 infection, compare the outcomes between KRT modalities in England during the first wave of the pandemic and estimate the excess mortality related to the pandemic. | Both dialysis and kidney transplant patients |
54,795 HHD: 1134 ICHD: 19 541 PD:2993 Transplant: 31 121 |
In a study of 2,783 individuals on kidney replacement therapy (KRT) who tested positive for SARS-CoV-2 out of 54,795 patients, mortality rates within 28 days were approximately 25% for in-centre hemodialysis and transplanted patients and 36% for those on home therapies. Mortality was higher in individuals aged 80 and above, lower for those aged 60-19, and lower in those listed for transplantation compared to those not listed. This underscores the extreme vulnerability of the KRT population to COVID-19, emphasizing the need for prioritized vaccination efforts. |
| Wilkinson et al. 2021 UK28 | Observational study | To investigate the impact of ethnicity and socioeconomic status on the severity of COVID- 19 outcomes specifically among individuals with chronic kidney disease (CKD) in the United Kingdom. | CKD/BAME | 459,042 10,480 had CKD at baseline. In those with CKD, the median age was 16.0 years, and 41.9% were males. Most of the CKD participants were White (94.2%) | The study found that individuals with CKD, especially BAME community, had a doubled risk of severe COVID-19, while socially deprived groups faced a 50-60% higher risk. Notably, CKD itself increased the risk of severe COVID- 19, regardless of ethnicity or deprivation, underscoring the need for targeted interventions and policy improvements to address health disparities in CKD patients. |
| Chang et al. 2021 USA30 | Observational study | To investigate the association between hospitalization for COVID-19 infection and various chronic conditions among Medicare beneficiaries, with a focus on racial and ethnic disparities. | BAME | 39.3 million | Racial/ethnic disparities persist in COVID-19 hospitalization rates among Medicare beneficiaries, with chronic conditions like CKD, acute myocardial infarction, heart failure, and diabetes linked to higher odds of hospitalization, emphasizing the need for targeted interventions in high- risk groups. |
| Swan et al. 2022 USA26 | Retrospective Cohort | To investigate and compare the clinical outcomes following hospital admission for COVID-19 management between patients with a history of solid organ transplant (SOT) and those without. | Solid organs transplant including kidney | The study included 4,562 patients who were hospitalized with COVID- 19, with 108 of them being solid organ transplant recipients and 4,454 as control patients. | Hospitalized solid organ transplant recipients required extended hospital stays but showed comparable short-term mortality outcomes from COVID- 19 to non-solid organ transplant recipients in a matched cohort, with a 60- day mortality rate of 11% versus 10% in the control group, suggesting a heightened mortality risk among transplant recipients. |
| Baptiste et al. 2023 USA16 | Propensity- matched cohort study | To examine the prevalence of COVID-19 in emergency room (ER) patients and investigate whether clinical outcomes varied by ESRD status. | ESRD patients | 27,106 | In the study, ESRD status did not increase the odds of testing positive for COVID-19. Among COVID-positive ER patients, ESRD was not independently associated with mortality, but ESRD patients exhibited a higher incidence of certain complications, including stroke, sepsis, and pneumonia, without an increase in overall adverse outcomes. |
| Patel el al. 2023 UK29 | A retrospective analysis | To investigate the association between comorbidities and COVID-19 outcomes. To identify and understand the relationships between common comorbidities (coronary heart disease, hypertension, type II diabetes mellitus, obesity, chronic kidney disease, depression, and anxiety) and the likelihood of contracting COVID-19 or experiencing severe outcomes, using data from the UK Biobank. | Patients with common comorbidities including CKD. | 472,182 | The study revealed that comorbidities increased the risk of COVID-19 infection and severity, particularly among BAME participants compared to White participants. The conclusion underscores the necessity of tailored interventions for individuals with specific comorbidities and the importance of addressing ethnic disparities in COVID-19 outcomes. |
AKI: Acute kidney injury, CKD: Chronic kidney disease, PCR: Polymerase chain reaction, ESRD: End-stage renal disease, BAME: Black, Asian and Minority Ethnic, HHD: Home hemodialysis, ICHD: In-centre hemodialysis, PD: Peritoneal dialysis, KRT: Kidney replacement therapy, ESKD: End-stage kidney disease, HD: Hemodialysis
Information was initially entered into the Summary Table by two authors (OE and IA). This was then checked, amended, and expanded where necessary by other reviewers (JB, VS, OA, AS, and NK). The quality of each article was evaluated using GRADE (Grades of Recommendation, Assessment, Development, and Evaluation) appraisal tools.
Outcome measures
The primary outcomes for CKD and CKD with kidney transplantation patients focused on incidence of COVID-19, mortality rates, hospitalization rates, and the need for intensive care. Secondary outcomes examined impact on dialysis and kidney transplantation patients. Disparities in COVID-19 outcomes were assessed by comparing BAME and non-BAME populations.
Results
The database search returned 373 articles, with 162 duplicates removed in the first phase, leaving 211 studies. After reviewing titles and abstracts, 159 articles were excluded, resulting in 52 for full-text review. Ultimately, 32 articles were deemed ineligible based on inclusion/exclusion criteria, leaving 20 papers included in the review. See Figure 1 PRISMA flow diagram for an overview of search results [Supplementary File 1].
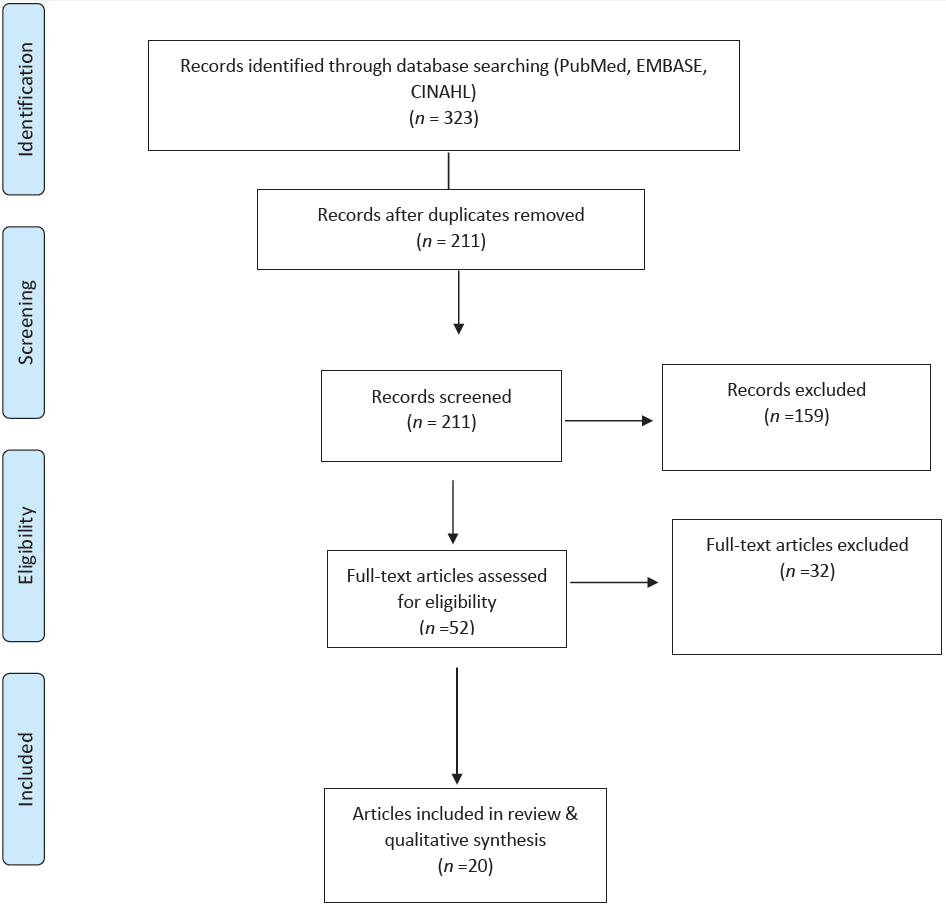
- PRISMA flow diagram highlighting the selection process for the studies included in the systematic review. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Among the 20 studies included in our review, six studies (1, 3, 5, 6, 15, and 19 in Table 2) focused on the effect of the COVID-19 pandemic on patients with CKD receiving dialysis services worldwide, and a further eight studies (4, 7–9, 12, 14, 15, and 18) focused on impacts of the virus on kidney transplant recipients and transplant programs. A group of seven studies (2, 10, 11, 13, 16, 17, and 20) focused on the impact of COVID-19 in BAME patients. A more detailed analysis is presented below.
Effect of COVID-19 on patients receiving dialysis
In a retrospective cohort study, Hsu et al.14 analyzed 7948 dialysis patients in the USA, revealing that 5.5% were infected with COVID-19. Reported risk factors included male sex, Black ethnicity, in-center dialysis, and comorbidities, with a mortality rate exceeding 20%. Salerno et al.15 undertook a similar study in the USA and they also identified that the COVID-19 infection rate and mortality among dialysis patients was significantly higher among the Black ethnic minority population and people who resided in a nursing home for an extended stay the previous year. Patients with CKD who had COVID-19 were also found to have higher incidence of stroke, sepsis, and pneumonia and higher hospital admissions and prolonged stays than non-CKD group during the pandemic. Black and Asian ethnic minorities, advanced age, and poor socioeconomic status were identified as significant independent predictor of death in the vulnerable ESRD group.16
Taji et al.17 examined COVID-19 disease characteristics and mortality for patients receiving long-term dialysis, comparing those infected with those who did not have the infection over a six-month period in Canada. They found an infection rate of 1.5% in 12,501 patients studied, about two-thirds (62.6%) of those with COVID-19 were admitted to the hospital, and the case fatality rate was 28.3%. In-center dialysis treatment, living in a long-term care residence, BAME, and low-income quintiles were identified as predictors of infection. In the UK, a retrospective study of renal registry data of people on kidney replacement therapy with COVID-19 by Savino et al.18 showed that a higher proportion of patients on home dialysis therapy (36%), both peritoneal and hemodialysis, died within four weeks of testing positive for SARS-CoV-2 compared with those on in-center dialysis therapy (25%). Also, age 80 years and above was associated with higher mortality, and patients from BAME populations were at a higher risk of infection compared to the White population. Khatri et al.19 studied 367 New York City hemodialysis patients, finding a 28% COVID-19 seropositive rate higher in the younger population, Black ethnic minority, and taxi users. The authors suggest the need for larger studies to confirm antibody efficacy.
Effect of COVID-19 on transplant programs and recipients
Elias et al.20 analyzed the incidence and clinical outcome of COVID-19 infection in kidney transplant recipients in France. Among the 1216 patients studied, 66 (5%) had COVID-19, which was higher than the incidence in the general population (0.3%). The mean age was 54.4 (SD 12.5) years, and a larger proportion was male (56%). The identified risk factors for infection were obesity, presence of comorbidities, and BAME. Mohan et al.21 report an analysis of the USA National Registry Data that found 11% of the 2020 waiting list patient deaths was attributed to COVID-19, with risks being male sex, obesity, and BAME. Active kidney transplant recipients have a 16% COVID-19 death rate, with risks such as young age, obesity, BAME, and lower education level. Similarly, Miller et al.22 reported a 37% higher mortality hazard in kidney transplant candidates in the post-COVID-19 National Emergency, particularly among Black ethnic minority waiting list candidates.
Lum et al.23 studied 41 kidney allograft patients with COVID-19, noting higher BAME representation. Hospitalization occurred in 64%, with a 9.8% mortality rate among intensive care unit (ICU) admissions. Analysis of US transplant recipient data revealed 384 COVID-19-related deaths among 131,659 patients, with mortality risk factors including age, obesity, male race, BAME, lower educational attainment level, and Medicaid insurance.24
Clarke et al.25 found excess mortality in solid organ transplant groups during the pandemic, with higher rates in kidney (188.5), lung (173.6), heart (123.7), and liver (105.1) per 10,000. BAME patients also had increased mortality. A study of hospitalization rate and survival of solid organ transplant recipients with COVID-19 in the year 2020 was undertaken by Swan et al.26 Analysis of data from 4562 patients hospitalized with COVID-19 compared 108 solid organ recipients with 4454 patients without solid organ transplants used as controls. Majority of the solid organ cohort received a kidney transplant (59%), and mortality at 60 days was higher in the solid organ transplant group compared with the control (17% SOT vs. 10 % control).
Differential impact of COVID-19 on BAME patients
Six studies highlighted the disproportionate impact of COVID-19 on BAME groups with CKD globally. Tabinor et al.,27 who undertook an observational study of 3379 patients on kidney replacement therapy in a single UK Renal Center, reported that 191 of them were infected with COVID-19 between March and April 2020. The BAME group accounted for 67%28 of the patients with COVID-19. Multivariate data analysis showed that BAME was associated with all-cause mortality after adjusting for age, deprivation, comorbidity, and frailty. The authors recommend development of strategies to improve BAME patients’ outcomes in a future outbreak of COVID-19. Wilkinson et al.28 examined the UK Biobank data of 459,042 participants, of whom 2.3% (10,480) had CKD. There were 5538 cases of severe COVID-19 among the patients whose data were retrieved, and of these, 4.5% occurred in those with CKD and 95.5% in those without CKD. Severe COVID-19 infection was more prominent in the BAME group than in their Caucasian counterparts. In participants with CKD, compared with the White group, BAME individuals were approximately 2.3 times more likely to have had severe COVID-19 (OR: 2.26; 95% CI: 1.34–3.80; P = 0.002) and those of South Asian ethnicity 2.1 times more likely (OR: 2.07; 95% CI: 1.07–4.00; P = 0.032). A similar pattern of association was observed in participants without CKD. In a subgroup analysis of the UK Biobank cohort study by Patel et al.,29 a stronger association was reported for certain comorbidities such as CKD, obesity, and diabetes mellitus among BAME participants than among their White counterparts. The study also found a statistically significant difference in the risk of COVID-19 diagnosis and severity between BAME and Caucasian participants. Chang et al.30 investigated COVID-19 hospitalization rates by race and ethnicity among Medicare patients in the USA during the pandemic. Their findings reinforce earlier reports of racial/ethnic disparity in the rate of hospitalization of COVID-19 patients with chronic medical conditions, including CKD. Corcillo et al.31 also reported a higher rate of hospitalization of ethnic minority patients among 39 consecutive CKD individuals admitted with COVID-19, identifying a 73% and 54% prevalence in renal transplant recipients and hemodialysis groups, respectively.
Research undertaken by Crews and Purnell32 identified fear and anticipated poor treatment as contributory factors to poor health-seeking behaviors among the BAME community in the USA during the pandemic, advocating trust-building during health crises. A review article by Long et al.33 closely examined the pathophysiology of COVID-19-associated kidney injury and its impact on long-term kidney function. The authors discussed the role of APOL 1 in contributing to the disproportionate burden of post COVID-19 kidney function decline among the ethnic minority group.
Discussion
This systematic review provides valuable insights into the global impact of COVID-19 on patients with CKD and kidney replacement therapy. Evidence on the differential impact on BAME patients, in terms of their health outcomes post COVID-19 infections, is also presented. The results indicate that COVID-19 has had a notable impact on patients undergoing hemodialysis and kidney transplant recipients. There is a less well-developed evidence base to demonstrate the impact of COVID-19 on dialysis services.
Several studies explored the incidence of COVID-19 and associated patient outcomes. Higher incidence, hospitalizations, need for intensive care services, and mortality rates are identified among patients undergoing hemodialysis compared to the general population, with a bidirectional relationship observed between COVID-19 and CKD, that is, CKD increases the risk of severe COVID-19 which, in its turn, leads to greater risk of acute and chronic kidney dysfunction.16,33 These studies confirm the higher level of clinical vulnerability of this population following infection.
Among hemodialysis patients, the main risk factors for COVID-19 infection included: male sex, old age, comorbidities, nursing home residence, commuting to dialysis centers with public transportation, and individuals in low-income quintiles.14,15,17–19 These findings underscore the intersectionality of socioeconomic and demographic factors in exacerbating health disparity within these vulnerable population during the pandemic. The reported disproportionate impact on the BAME hemodialysis population may reflect underlying systemic inequality in healthcare access and quality, compounded by factors such as language barriers and cultural differences in health-seeking behaviors.10,14,24 The critical role of socioeconomic status in shaping exposure risk may be linked to individuals from low-income quintiles facing greater difficulties adhering to preventive measures or reliance on public transportation for dialysis increasing their vulnerability. The clustering of these risk factors suggest a multifaceted health service challenge in protecting hemodialysis patients from COVID-19 necessitating targeted public health interventions that address both medical and social determinants of health.
Among kidney transplant recipients, including those on waiting lists, there is a similar evidence of higher rates of COVID-19, greater numbers of hospital admissions, and increased mortality rates compared to the general population.26 Individual risk factors associated with higher mortality rates among this group of patients are similarly male sex, advancing age, obesity, presence of comorbidities, the requirement for intensive care support, lower educational attainment, and BAME group.20,21
In general, for people with CKD, the review highlights the disproportionate burden borne by BAME patients, who exhibit increased rates of severe infection and mortality compared to their Caucasian counterparts. There is also evidence of significant increases in the duration of hospital stays, need for mechanical ventilation support, incidence of acute kidney injury, requirement for continuous kidney replacement therapy, and in-hospital mortality. Factors that may contribute to this disparity, depending on the country, may be poverty, lack of healthcare access, being uninsured, using public transportation, frontline occupations, and crowded living environments, in addition to cultural and ethnic factors. Health-seeking behaviors among the BAME population might also play a role in this disparity.30,32
This review has also identified potential biological contributing factors to these disparities, including the influence of genetic predisposition such as APOL-I variants. However, despite these insights; several gaps in knowledge persist. For instance, additional research is warranted to elucidate the underlying mechanism driving the observed disparities, including the interplay of genetic, socioeconomic, and environmental factors.34,35
There are a few limitations to our systematic review. The relative importance of different risk factors for poor outcome remains unclear. Studies from Africa, South America, and Asia were underrepresented, possibly due to the English language limiter. Finally, the studies identified were highly heterogeneous in terms of study design, population, and outcomes measured, which made it impossible to pool data from individual studies to increase power and precision of estimates of observed effects.
These review findings underscore the general need for tailored interventions and policies to address the heightened vulnerability of BAME populations, especially those with CKD and those on kidney replacement therapy, and prevent future adverse COVID-19 outcomes. Clinicians should prioritize tailored interventions to ensure equitable access to healthcare, culturally sensitive communication, and targeted support for at-risk groups. Policy-makers must address social determinants of health and implement strategies to mitigate health disparities, promoting health equity.
In the future, special attention and care should be directed toward protecting vulnerable populations from future pandemics, emphasizing evidence-based approaches and global equity in healthcare access.
This systematic review is the first review as far as we are aware that provides evidence from high-quality studies on how the COVID-19 pandemic affected people with CKD on hemodialysis and those living with kidney allografts. Our findings demonstrate that the presence of CKD in patients with COVID-19 was a prognostic factor for poor patient outcome, along with obesity, lower socioeconomic group, and BAME population group. A similar pattern was observed among transplant patients and those on the transplant waiting list. When compared with White majority patients, morbidity and mortality were both higher in BAME cases as well as the severity and existence of aggravating COVID-19 complications.
Acknowledgment
The authors would like to thank Dr. Anil Gumber and Professor Mark Johnson, who both contributed to the initial scoping review.
Data availability
The articles used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of interest
There are no conflicts of interest.
References
- Triadic dimensionalities: Knowledge, movement, and cultural discourse—in the wake of the covid-19 pandemic. Int J Semiot Law. 2022;35:823-30.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- COVID-19: Immunopathology and its implications for therapy. Nat Rev Immunol. 2020;20:269-70.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Update in renal transplantation. Arch Intern Med. 2004;164:1373-88.
- [CrossRef] [PubMed] [Google Scholar]
- Systematic review: Kidney transplantation compared with dialysis in clinically relevant outcomes. Am J Transplant. 2011;11:2093-109.
- [CrossRef] [PubMed] [Google Scholar]
- Comparative survival and economic benefits of deceased donor kidney transplantation and dialysis in people with varying ages and co-morbidities. PLoS One. 2012;7:e29591.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Et DG, Martín C. Newsletter Transplant International figures on donation and transplantation Produced By The Council of Europe European Committee (Partial. Vol. 23. 2018. https://www.edqm.eu/en/-/just-released-newsletter-transplant-2018#:∼:text=The%20Newsletter%20Transplant%20provides%202017%20figures%20and%20analysis%20of%20international
- Managing the COVID-19 pandemic: International comparisons in dialysis patients. Kidney Int. 2020;98:12-6.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- COVID-19 of dialysis patients in Japan: Current status and guidance on preventive measures. Ther Apher Dial. 2020;24:361-5.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Transplant programs during COVID-19: Unintended consequences for health inequality. Am J Transplant. 2020;20:1954-5.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Prats-Uribe A, Paredes R, Prieto-Alhambra D, Prats Uribe A. Ethnicity, comorbidity, socioeconomic status, and their associations with COVID-19 infection in England: A cohort analysis of UK Biobank data. medRxiv. 2020;2020.05.06.20092676. Available from: https://www.medrxiv.org/content/10.1101/2020.05.06.20092676v3%0Ahttps://www.medrxiv.org/content/10.1101/2020.05.06.20092676v3.abstract [Last accessed on 2024 Jun 01].
- von Hagen A, Balbi A, Arbildi C, Bonilla M. International prospective register of systematic reviews citation review question participants/population intervention(s), exposure(s) comparator(s)/control main outcome(s) international prospective register of systematic reviews additional. Int Prospect Regist Syst Rev 2018;1–4. Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020152975 [Last accessed on 2024 Jun 01].
- Defining and designing mixed research synthesis studies. Res Sch. 2006;13:29.
- [PubMed] [PubMed Central] [Google Scholar]
- The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021;18:e1003583.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- COVID-19 among US dialysis patients: Risk factors and outcomes from a national dialysis provider. Am J Kidney Dis. 2021;77:748-56.e1.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- COVID-19 risk factors and mortality outcomes among Medicare patients receiving long-term dialysis. JAMA Netw Open. 2021;4:e2135379.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Prevalence and predictors of outcomes among ESRD patients with COVID-19. BMC Nephrol. 2023;24:67.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- COVID-19 in patients undergoing long-term dialysis in Ontario. CMAJ. 2021;193:E278-84.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Outcomes of patients with COVID-19 on kidney replacement therapy: A comparison among modalities in England. Clin Kidney J. 2021;14:2573-81.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- COVID-19 antibodies and outcomes among outpatient maintenance hemodialysis patients. Kidney360. 2020;2:263-9.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- COVID-19 infection in kidney transplant recipients: Disease incidence and clinical outcomes. J Am Soc Nephrol. 2020;31:2413-23.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- COVID-19-associated mortality among kidney transplant recipients and candidates in the United States. Clin J Am Soc Nephrol. 2021;16:1695-703.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Mortality among solid organ waitlist candidates during COVID-19 in the United States. Am J Transplant. 2021;21:2262-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Spectrum of coronavirus disease 2019 outcomes in kidney transplant recipients: A single-center experience. Transplant Proc. 2020;52:2654-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- COVID-19 mortality among kidney transplant candidates is strongly associated with social determinants of health. Am J Transplant. 2021;21:2563-72.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Excess mortality among solid organ transplant recipients in the United States during the COVID-19 pandemic. Transplantation. 2022;106:2399-407.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Hospitalization and survival of solid organ transplant recipients with coronavirus disease 2019: A propensity matched cohort study. PLoS One. 2022;17:e0278781.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- End-stage kidney disease patients from ethnic minorities and mortality in coronavirus disease 2019. Hemodial Int. 2022;26:83-93.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Association of ethnicity and socioeconomic status with COVID-19 hospitalization and mortality in those with and without chronic kidney disease. Kidney Int Rep. 2022;7:334-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Comorbidities associated with the severity of COVID-19, and differences across ethnic groups: A UK Biobank cohort study. BMC Public Health. 2023;23:1566.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- COVID-19 hospitalization by race and ethnicity: Association with chronic conditions among Medicare beneficiaries, January 1–September 30, 2020. J Racial Ethn Health Disparities. 2022;9:325-34.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- High prevalence of Afro-Caribbean ethnicity and hypoglycaemia in patients with diabetes and end stage renal disease hospitalized with COVID-19. Nephrology (Carlton). 2021;26:252-4.
- [CrossRef] [PubMed] [Google Scholar]
- COVID-19, racism, and racial disparities in kidney disease: Galvanizing the kidney community response. J Am Soc Nephrol. 2020;31:1-3.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- COVID-19 survival and its impact on chronic kidney disease. Transl Res. 2022;241:70-82.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Pathophysiology of COVID-19-associated acute kidney injury. Nat Rev Nephrol. 2021;17:751-64.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- APOL1 nephropathy: From genetics to clinical applications. Clin J Am Soc Nephrol. 2021;16:294-303.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




