

Translate this page into:
Fetuin-A and vascular calcification in Indian end-stage renal disease population
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Fetuin-A levels, its correlation with vascular calcification and other biochemical markers of chronic kidney disease-mineral and bone disorder (CKD-MBD) has not been studied in Indian end-stage renal disease population. Forty patients on dialysis for more than 3 months were studied. Biochemical parameters of CKD-MBD, highly sensitive-C reactive protein (hs-CRP), lipid profile and fetuin-A levels were estimated. Multi-slice computed tomography (MSCT) at the level of L1–L4 was done, and calcification score calculated using AJ 130 smart score. Levels of fetuin-A were correlated with calcification score and biochemical markers of CKD–MBD. Mean fetuin-A levels were 0.33 ± 0.098 g/l. Positive correlation of abdominal aortic calcification scores was found with age (P < 0.01) and duration of dialysis (P = 0.018). No correlation was detected between MSCT score, calcium phosphate product, intact parathyroid hormone, vitamin D, triglycerides and fetuin-A, and there was no correlation between fetuin-A levels, age, dialysis duration and calcium phosphate product but a significant correlations with vitamin D3 (P = 0.034), serum albumin (P = 0.002) was detected. Inverse correlation with hs-CRP was obtained. Patients with ischemic heart disease had numerically lower levels of fetuin-A (P = 0.427) and numerically higher MSCT score (P = 0.135). Patients with low hs-CRP (<10) had numerically higher fetuin-A levels (P = 0.090) and significantly low MSCT scores (P = 0.020). Calcium deposition seen on MSCT increases with age and duration of dialysis but is not related to fetuin-A levels. Inconclusive relationship exists with other parameters of CKD-MBD. Large controlled studies are needed to establish the role of fetuin-A in vascular calcification in Indian population.
Keywords
Abdominal aorta calcification
end-stage renal disease
fetuin-A
India

Introduction
Disturbances in mineral metabolism and bone disease are common complications of chronic kidney disease (CKD) and an important cause of morbidity and decreased quality of life. Importantly, there is increasing evidence suggesting that these disorders in mineral and bone metabolism are associated with increased risk of cardiovascular (CV) calcification, morbidity, and mortality.[1]
Recent basic and clinical data support the notion that vascular calcification such as skeletal osteogenesis is an active cell-mediated process that is regulated by various calcification Inducers and inhibitors. Evidence suggests that the interaction of traditional (i.e., framingham: Age, lifestyle, diabetes, hypertension, dyslipidemia) and uremia related (e.g., hyperphosphatemia, high calcium phosphorus product, hyperparathyroidism, oxidative stress, systemic inflammation, protein energy wasting, asymmetrical dimethylarginine, p-cresol, fetuin-A) CV risk factors contribute to excessive and accelerated vascular calcification in CKD patients.[2]
Fetuin-A, 62 kDa hepatocyte derived acute phase glycoprotein, is one of the most powerful circulating inhibitors of hydroxyapatite formation.[3] In patients with end-stage renal disease (ESRD), its circulating levels are significantly reduced.[45] It is not clear whether fetuin-A deficiency is a predictor of vascular calcification leading to vascular stiffness in dialysis patients. So, we planned to do a study to measure fetuin-A level in end-stage renal disease patients and evaluate the correlation between multi-slice computerized tomography (MSCT) calcium score and various biochemical parameters of CKD mineral and bone disorder.
There are no studies to find out the correlation between aortic vascular calcification scores and fetuin-A particularly in Indian ESRD patients so far. We present the findings of our study to evaluate correlation.
Materials and Methods
This cross-sectional study was conducted on 40 patients of ESRD at a tertiary care hospital in India. The study protocol was approved by Institute Ethics Committee, and study was conducted according to principles mentioned in Declaration of Helsinki. Written informed consent was obtained from all patients before subjecting them to any procedure.
End-stage renal disease patients on dialysis for at least 3 months were included. Patients with co-existing hepatic failure, active infection, fracture or those unwilling to participate in the study were excluded. Included patients were subjected to MSCT at L1–L4 vertebrae for aortic artery calcification and biochemical investigations for serum calcium, phosphate, fetuin-A, parathyroid hormone, Vitamin D3, albumin, highly sensitive-C reactive protein (hs-CRP) and calcium phosphorus product. Additionally, lipid profile and ESR were also done. Fetuin-A levels were measured using internationally standardized kit by BioVendor Research and diagnostic products. The blood samples for fetuin-A were centrifuged at 6000 rpm for 5 min and serum stored in deep freezer at −80°C until analyzed in duplicate, and average values were recorded. Vitamin D3 levels were done using radioimmunoassay technique. Intact parathyroid assay was done by sandwich immunoassay using chemiluminometric technology, which uses constant amounts of anti-human parathyroid antibodies in the lite reagent. The assay for hs-CRP was based on particle enhanced turbidimetric immunoassay technique. All biochemical investigations were done at National Accreditation Board for Testing and Calibration Laboratories certified laboratory.
Calcium scoring
It was done using GE 64 slice VCT-XT computed tomography machine on nondialysis day. Software used was Smart score (AJ 130 score). Technically patient was placed supine position with anatomical reference of xiphisternum. Serial cuts of 0.625 mm were obtained at the level of L1–L4, and calcium score was calculated using AJ 130 (Smart score).
Statistical analysis
The data were analyzed using SPSS software (version 16) IBM Inc., USA. Descriptive statistics was applied to demographic variables, radiological and biochemical parameters. For comparison of normally distributed quantitative variables, Pearson correlation was used. For comparing quantitative variables that were normally distributed between groups, independent t-test was used (assuming alpha = 0.05 and power 80%). For variables that were not normally distributed, nonparametric tests were employed that is, Spearman Rho and Mann–Whitney U-test. P < 0.05 was considered as statistically significant.
Results
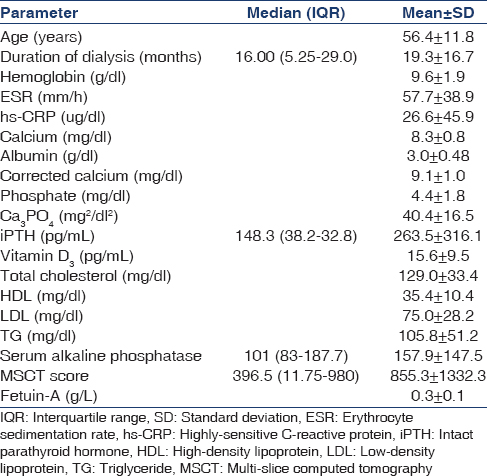
The mean age of patients in the study group was 56.7 ± 11.8 years. The duration of dialysis in months was 19.3 ± 16.7 months. Most common reason for patients undergoing dialysis was diabetic nephropathy (47.5%) followed by chronic glomerulonephritis (30%). The minimum duration of dialysis was 3 months and the maximum duration was 66 months. Demographic and biochemical features of patients enrolled in the study are given in Table 1.
Vitamin D deficiency was present in 37 of the 40 patients. Further, the study population was divided into mild, moderate and severe deficiency, defined by KDIGO as 16–30 pg/ml, 6–15 pg/ml and <5 pg/ml respectively. Severe Vitamin D3 deficiency was found in 5 patients whereas 16 patients each had mild and moderate deficiency.
Correlation of multi-slice computerized tomography score with other parameters
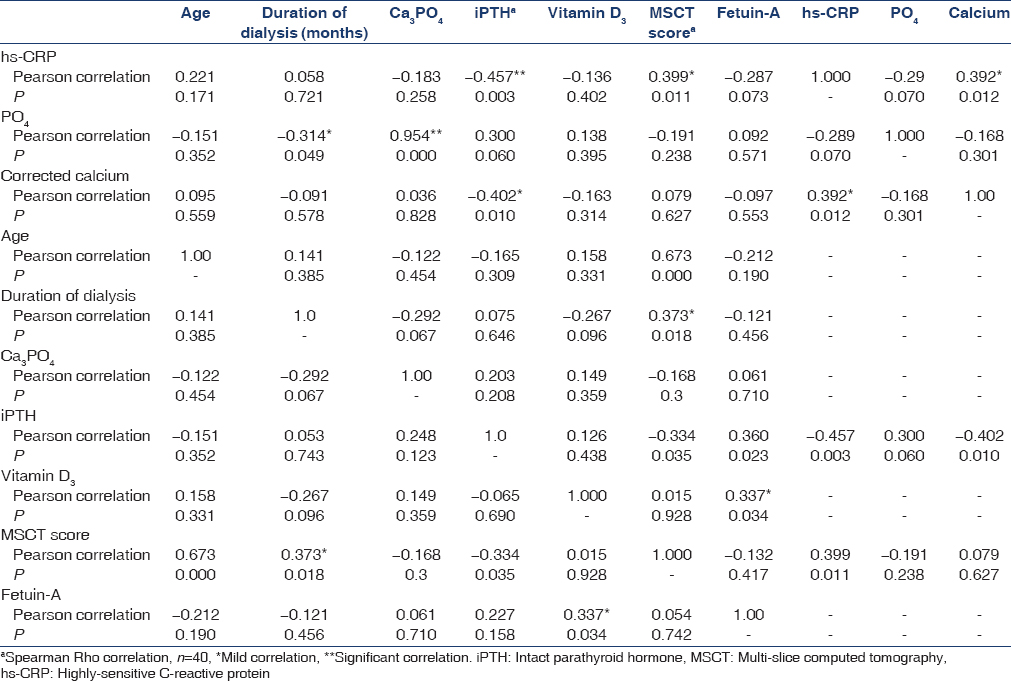
Multi-Slice Computerized Tomography score was correlated with other parameters using t2-test. A positive correlation was found with age (r = 0.67; P < 0.001) and duration of dialysis (r = 0.3; P = 0.01). Figures 1 and 2 show the correlation between MSCT score with age of patient and fetuin-A levels.

- Correlation of Multi-slice computed tomography score with age

- Correlation of Multi-slice computed tomography score with fetuin-A level
There was no correlation between MSCT score and calcium phosphate product, intact parathyroid hormone, Vitamin D3, triglyceride and serum fetuin-A levels. There was also a nonsignificant positive correlation with intact parathyroid hormone (iPTH) [Table 2].
Fetuin-A and various biochemical parameters
The serum fetuin-A levels were correlated with various parameters such as age, duration of dialysis, calcium phosphate product, parathyroid hormone, Vitamin D3, triglyceride, albumin and highly sensitive C reactive protein(CRP). There was no correlation with age, duration of dialysis and calcium phosphate product. There was statistically significant correlation with Vitamin D3 (0.337, P = 0.034). When serum fetuin-A was correlated with serum albumin, a significant correlation was obtained (0.466, P = 0.002). There was nonsignificant inverse correlation between fetuin-A and hs-CRP [Table 2].
Sub-group analysis
Ischemic heart disease
The patients with ischemic heart disease (IHD) had lower value of serum fetuin-A as compared to the patients without ischemic heart disease (0.32 vs. 0.35, P = 0.427). Similarly, the patients with IHD had higher MSCT calcium scores, which were statistically insignificant. There was no significant difference between these two groups when Ca3PO4, iPTH, Vitamin D3, cholesterol, high-density lipoprotein, low-density lipoprotein and albumin were compared. Table 3 shows the results of sub-group analysis.

Diabetes mellitus
Serum values of fetuin-A and MSCT calcium score were correlated using t-test and Spearman Rho test in diabetics and nondiabetic patients. Diabetic patients had high MSCT values and lower values of fetuin-A, which was not statistically significant.
Patients with high and low highly sensitive-C reactive protein values
The values of serum fetuin-A and MSCT score were further divided into two separate groups based on the values of hs-CRP (<10 ug/dl vs. >10 ug/dl). These groups thus obtained were compared with each other. The serum value of fetuin-A was higher in patients with low hs-CRP. Similarly, patients with low CRP had low values of MSCT scores, which were statistically significant (P = 0.02).
Discussion
Calcifying atherosclerosis is an active process, which is controlled by calcification inhibitors and inducers. It is prevalent in dialysis patients and is associated with a high burden of CV disease. Fetuin-A, an acute phase glycoprotein, is one of the most powerful circulating inhibitors of hydroxyapatite formation. This study was a cross-sectional study conducted on forty dialysis patients. Our study is the first study conducted in Indian end-stage renal disease patients to find out the correlation between serum fetuin-A and MSCT calcium scores in aorta. The study was planned to evaluate the correlation between MSCT calcium score and various biochemical and patients parameters.
Our study found out that as the duration of dialysis and age increases, the calcium score calculated by MSCT at the level of L1–L4 also increases. We found an inverse correlation with iPTH. Our results matched with CORD study where they found out that independent predictors for the presence and severity of calcification were age (odds ratio [OR] = 1.103/year; P < 0.0001), duration of dialysis (OR = 1.110/year; P = 0.002) and history of CV disease (OR = 3.247; P < 0.0001).[6]
In another study, association between pelvic arterial calcification and arteriovenous thigh graft failure was studied and patients with high and low calcium scores were evaluated. It was found that the vascular calcification was severe in male gender and older age. The duration of dialysis, phosphate levels, parathyroid hormone, calcium phosphorus product, serum alkaline phosphate did not differ between two groups. Our study concluded that calcification is dependent on age, iPTH and is not related to phosphate levels, parathyroid hormone, calcium phosphorus product or serum alkaline phosphatase.[7]
In various studies evaluating epidemiological and biochemical risk factors for calcification, age was the most consistent factor for calcification whereas diabetes, time on dialysis, male gender, high serum iPTH/ALP levels, hyperphosphatemia and increased Calcium phosphorus product were identified in some studies, but the latter relationships could not be uniformly reproduced.[8]
Our study was also aimed to establish a correlation between serum fetuin-A and MSCT calcium score. We could not establish any significant correlation between these two variables. Fetuin-A levels were inversely correlated with serum hs-CRP and positive correlation with serum albumin and Vitamin D3.
In most but in all studies, fetuin-A has been found to be having a negative correlation with rates of vascular calcification. Fetuin-A levels are significantly lower in dialysis patients, and this has been correlated with higher rates of vascular calcification, CV mortality, malnutrition and inflammation states as assessed by subjective global assessment and CRP levels. Hypoalbuminemia has also been found to strongly related to fetuin-A deficiency, suggesting expected involvement in malnutrition-inflammation-atherosclerosis syndrome in clinical fetuin-A deficiency. Results of these studies suggest fetuin-A as both a calcification inhibitor protein and a negative acute phase reactant as a link between inflammation atherosclerosis in patients with CKD.[4910]
Zheg et al., studied the relation of serum fetuin-A and coronary artery calcium score (CACS) in African American patients, showed that only fetuin-A was significantly associated with CACS, which was not so in our study.[11] In a study by Oikawa et al., on 40 hemodialysis patients, there was a negative correlation between serum fetuin-A levels and duration of dialysis, BNP, and hs-CRP, and a positive association with serum albumin. The results of this are comparable to our study where there is a negative correlation between duration of dialysis (r = −0.121. P = 0.456), hs-CRP and a positive correlation between serum albumin (r = −0.287, P = 0.073).[12] Almost similar results were obtained by Hermans et al., in their study as well.[5] In a recent study evaluating various risk factors (matrix Gla protein, osteopontin, osteoprotegerin, pyrophosphates, fetuin-A) for calcification of coronary arteries and abdominal aorta, only osteoprotegerin was associated with calcification.[2]
In many studies, feuin-A levels have been found to be inversely correlated with CRP, emphasizing its nature as negative acute phase reactant. Hypoalbuminemia has also been found to strongly related to fetuin-A deficiency, suggesting expected involvement in malnutrition-inflammation-atherosclerosis syndrome in clinical fetuin-A deficiency.[13]
Though most of the studies have found a significant correlation between fetuin-A levels and vascular calcification, our study could not establish the same. There could be various possible reasons for this. Firstly, we have not included any controls – we need to have controls for Indian population both for MSCT abdominal aortic calcium and serum fetuin-A. The effect of genetic variations of the gene encoding fetuin-A is not studied in Indian population. Indians can have different fetuin-A gene coding for different product. This effect of variations in gene encoding fetuin-A on CV mortality and morbidity was studied by Stenvinkel et al. in hemodialysis patients.[10] He found out that the patients with α2-Heremans schmid glycoprotein 256Ser allele had lower serum fetuin-A levels and higher all cause CV mortality if they were inflamed. So, the effects of these genetic variations on Indian population need further investigations. The lower fetuin-A levels in our study could be due to genetic variability. Secondly, cross-sectional nature of our study which assessed fetuin-A levels at only one point of time could have missed changes in the serum levels. This may also be the reason that we could not find a correlation between vascular calcification and fetuin-A. Thirdly, the values of certain variables like MSCT scores, iPTH, hs-CRP were not in range. They had very high and very low values which could be due to shorter duration of dialysis and have skewed our results to the either side. For example, some patients (9 patients) did not have any vascular calcification at all and one patient had extremely high value of MSCT. In addition, we did not use volumetric analysis of calcium deposition in aorta though Agatston score used here has been recommended and standardized for this type of study, but volumetric analysis of calcium deposition can influence the results.
We further divided the study group on the basis of presence and absence of IHD. We found out that the patient with IHD had lower value of serum fetuin-A and higher MSCT calcium scores which were statistically insignificant. Similarly, we detected statistically insignificant higher values of CRP in patients with IHD. However, CORD study found that the patients with a history of CVD had statistically significant higher abdominal aortic calcium (AAC) scores.[6]
Wilson et al., studied the paramount importance of AAC in predicting the vascular morbidity and mortality. They found that the presence of AAC was generally associated with increased risk of CV mortality and morbidity. Our study though did not follow up the patients for the CV events, it did found out that the patients with a history of ischemic/coronary heart disease did have higher calcium aortic scores.[14]
Our study had several limitations. First, our study population was not randomized. There were several variances in the study population like diabetic versus nondiabetics, duration of dialysis, poor calcium and phosphate control, which require randomization. Second, even the values of certain variables such as MSCT scores, iPTH, hs-CRP were not in range. They had very high and very low values, which could have skewed our results to the either side. Third, we have not used volumetric analysis of calcium deposition in aorta, though Agatston score used here has been recommended and standardized for this type of study, but volumetric analysis of calcium deposition can influence the results. Fourth, we have not included any controls – we need to have controls for Indian population both for MSCT abdominal aortic calcium and serum fetuin-A.
Taking into account the above-mentioned limitations, we need further larger studies to establish the role of fetuin-A in vascular calcification specially in Indian ESRD patients. But, it is to note that ours is the first study in Indian ESRD patients using MSCT to score the calcification, and it does state that abdominal aortic calcification increases as the age and duration of dialysis increase and patients with higher inflammation (hs-CRP ≥10) have higher calcification scores.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Morbidity and mortality associated with abnormalities in bone and mineral metabolism in CKD. In: Clinical Guide to the Basics of Bone and Mineral Metabolism in CKD. New York: National Kidney Foundation; 2006. p. :77-92.
- [Google Scholar]
- Calcification of coronary arteries and abdominal aorta in relation to traditional and novel risk factors of atherosclerosis in hemodialysis patients. BMC Nephrol. 2013;14:10.
- [Google Scholar]
- The serum protein alpha 2-Heremans-Schmid glycoprotein/fetuin-A is a systemically acting inhibitor of ectopic calcification. J Clin Invest. 2003;112:357-66.
- [Google Scholar]
- Association of low fetuin-A (AHSG) concentrations in serum with cardiovascular mortality in patients on dialysis: A cross-sectional study. Lancet. 2003;361:827-33.
- [Google Scholar]
- Association of serum fetuin-A levels with mortality in dialysis patients. Kidney Int. 2007;72:202-7.
- [Google Scholar]
- Abdominal aortic calcification in dialysis patients: Results of the CORD study. Nephrol Dial Transplant. 2008;23:4009-15.
- [Google Scholar]
- Association of pelvic arterial calcification with arteriovenous thigh graft failure in haemodialysis patients. Nephrol Dial Transplant. 2004;19:2564-9.
- [Google Scholar]
- KDIGO clinical practice guidelines for diagnosis, evaluation, prevention and treatment of chronic kidney diseae – Mineral bone disease (CKD-MBD) Kidney Int. 2009;113(Suppl 16):S47.
- [Google Scholar]
- Serum albumin, C-reactive protein, interleukin 6, and fetuin A as predictors of malnutrition, cardiovascular disease, and mortality in patients with ESRD. Am J Kidney Dis. 2006;47:139-48.
- [Google Scholar]
- Low fetuin-A levels are associated with cardiovascular death: Impact of variations in the gene encoding fetuin. Kidney Int. 2005;67:2383-92.
- [Google Scholar]
- Relation of serum fetuin-A levels to coronary artery calcium in African-American patients on chronic hemodialysis. Am J Cardiol. 2009;103:46-9.
- [Google Scholar]
- Evaluation of serum fetuin-A relationships with biochemical parameters in patients on hemodialysis. Clin Exp Nephrol. 2007;11:304-8.
- [Google Scholar]
- Abdominal aortic calcific deposits are an important predictor of vascular morbidity and mortality. Circulation. 2001;103:1529-34.
- [Google Scholar]




