

Translate this page into:
Interpretation of Kidney Biopsy in Indian Patients Older than 60 Years: A Tertiary Care Experience
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The adult population above the age of 60 years has significantly increased in India, with a life expectancy of 68.4 years in 2016. Data regarding the renal histopathology in these patients are scarce though the number of native kidney biopsies done in this subset of population is increasing. The present study is a retrospective analysis of 231 biopsies from a total of 700 biopsies, from patients above 60 years of age (M = 65.8%; F = 34.2%) with a mean age of 64 ± 6.03 years. The indications for kidney biopsy included nephrotic syndrome (NS) (30.4%), nephritic syndrome (19.1%), rapidly progressive renal failure (11.7%), acute kidney injury (AKI) (15.7%), and acute worsening of preexisting chronic kidney disease (CKD) (23%). The median percentage of glomerulosclerosis was 22% (5%–45%), and interstitial fibrosis and tubular atrophy was 30% (10%–50%). The most common cause for nephrotic syndrome was membranous nephropathy (31.4%) and for nephritic syndrome was benign arterionephrosclerosis (22.7%). Postinfectious glomerulonephritis (29.6%) was the leading cause for rapidly progressive renal failure. Acute injury on CKD was notable in patients with diabetic nephropathy (30.2%). The predominant causes for AKI were acute tubulointerstitial nephritis (33.3%), acute tubular necrosis (22.2%), and acute pyelonephritis (19.4%). The biopsy proven histopathological features enabled us in tailoring the therapy. None of the patients developed life-threatening complications following ultrasonography-guided biopsy.
Keywords
Elderly
kidney biopsy
pattern of biopsy

Introduction
India being the second most populous country in the world, adults above 60 years, comprises about 10-13% of the total population.[1] As the geriatric population is increasing, concurrent illness leading to kidney disease is more prevalent. Majority of the chronic kidney disease (CKD) patients as per the findings of the CKD registry of India cannot afford renal replacement therapy.[2] The spectrum of renal diseases in this subpopulation differs from that in the younger population in terms of acute kidney injury (AKI) and CKD.[3] Diabetes being the most common cause of CKD, a kidney biopsy is indicated only in a subset of the patients for appropriate diagnosis and management. Reversible causes such as primary/secondary glomerulonephritis (GN), acute tubulointerstitial nephritis, and other acute injuries can be diagnosed in difficult situations with the help of an adequate kidney biopsy specimen.
The management and prognosis of renal diseases vary in this subpopulation. The use of immunosuppressive agents, discontinuation of nephrotoxic drugs, treatment of infection, and renal replacement therapy are routinely used in patients above 60 years as per the indications. More focused data have been published recently on the role of kidney biopsy and the clinicopathologic correlation in adults above 60 years.[456] To the best of our knowledge, there is a paucity of large database available on the histopathological spectrum in elderly above 60 years from India.
The aim of this study is to analyze the histopathological spectrum of native kidney biopsies in elderly patients (>60 years) from a tertiary care center in South India.
Materials and Methods
This retrospective study was conducted in coordination with the Departments of Nephrology and Pathology of Madras Medical Mission, Chennai, India, from January 2010 to August 2016. All patients above the age of 60 years, who had an indication to do kidney biopsy, were counseled by the treating nephrologist and a written consent was obtained for the biopsy. Small sized kidneys with complete loss of corticomedullary differentiation, polycystic kidney disease and those with hydronephrosis were excluded from the study. Those who were on aspirin, clopidogrel, or anticoagulants were biopsied after the discontinuation of the drug and appropriate time interval. All biopsies were conducted under ultrasonography (USG) guidance by a trained nephrologist with the use of local anesthesia. Blood pressure was adequately controlled before biopsy in those patients who were taking antihypertensive drugs. The site of the kidney biopsy, either right or left, was decided by the nephrologist, with the help of real-time USG examination. A biopsy gun was used, and the specimen was collected for light microscopy, immunofluorescence, and electron microscopy in a few biopsies for confirmation of glomerulonephritis. The patients were discharged home after observation for 6–8 h in the day care. Those who had macroscopic hematuria were admitted overnight and discharged the next day when the urine was clear.
Two cores of renal tissue were sent to the histopathology laboratory, one in 10% formalin and the other in Michel's transport media. The paraffin-embedded tissue was stained for H and E, PAS, PASM, and trichrome stains. Additional stains, such as Congo red, were conducted when indicated. For immunofluorescence, the fresh tissue was stained with antibodies – IgG, IgM, and IgA, complements – C3 and C1q, and light chains – kappa and lambda. In cases of membranous nephropathy (MN), staining for antiphospholipase A2 receptor in serum or tissue could not be performed.
The main clinical syndromes requiring kidney biopsy were as follows:
-
Nephrotic syndrome (NS) defined as proteinuria >3.5 g/day and hypoalbuminemia (<30 g/L) with clinical evidence of generalized edema
-
Chronic GN defined as proteinuria and/or hematuria for >3 months
-
AKI was defined according to the KIDGO guidelines (2012).
Data included demographic data, clinical, and histopathological findings. Statistical analysis was carried out using SPSS 16 platform. The percentages or mean and standard deviation were used to describe categorical and continuous variables. Differences of qualitative data were compared using the Chi-square test/Fisher's exact test. The Student's t-test was used to compare continuous variables. A P< 0.05 was considered statistically significant.
Results
Of a total 700 native kidney biopsies between January 2010 and August 2016, 231 biopsies were conducted in patients above 60 years of age (M = 152; F = 79). The mean age of the patients was 64.2 ± 6.03 years. The oldest patient who underwent a renal biopsy was 82 years. Demographic data of the patients above 60 years undergoing native kidney biopsy are shown in Table 1. The indications for kidney biopsy are shown in Figure 1. The median percentage (IR) of global glomerulosclerosis and interstitial fibrosis and tubular atrophy diagnosed in the renal tissue of the elderly were 22% (5%–45%) and 30% (10%–50%), respectively. The most common histopathological diagnosis seen in our series was diabetic nephropathy (14.3%), followed by chronic tubulointerstitial nephritis (11.3%) and membranous nephropathy (MN) (10.4%). One biopsy had minimal histologic abnormality [Figure 2].


- Indication to biopsy
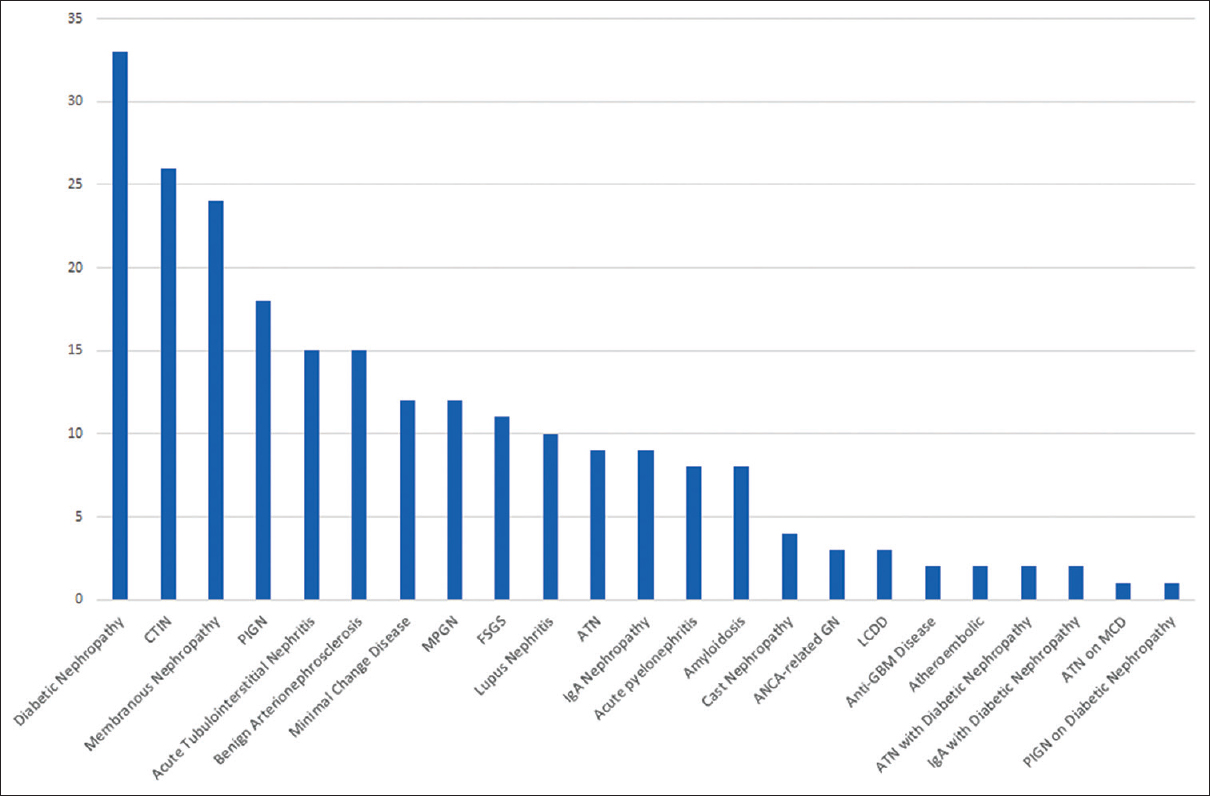
- Histological diagnosis
The commonest cause for NS were MN (31.4%). Secondary causes for MN were clinically assessed. The causes for nephritic syndrome were benign arterionephrosclerosis (22.7%) followed by IgA nephropathy (20.5%), postinfectious glomerulonephritis (PIGN) (18.2%), and membranoproliferative glomerulonephritis (18.2%). The leading cause for RPRF was PIGN (29.6%) and lupus nephritis (18.5%). Chronic tubulointerstitial nephritis (45.3%) and diabetic nephropathy (30.2%) were the most common histopathological findings seen in patients with acute worsening of a preexisting CKD. Acute tubulointerstitial nephritis (33.3%), acute tubular necrosis (ATN) (22.2%), and acute pyelonephritis (19.4%) were the most common cause of AKI, in our study population, as shown in Figure 3. Acute pyelonephritis was diagnosed with correlation to urine analysis findings.

- Percentage of renal diseases in the various clinical syndromes
About 100% patients had microhematuria following kidney biopsy. No patient had major bleeding episodes post kidney biopsy. One patient developed hypotension post biopsy, which responded to intravenous fluids.
Discussion
To the best of our knowledge, there is little data about the pattern of biopsy-proven kidney diseases in adult patients above 60 years from South India. In the current study, we analyzed the clinical and pathological data of 700 cases getting kidney biopsies from January 2010 to August 2016, in a tertiary care center from South India, in which the adults above 60 years constituted about 30%. In this cohort, we found that NS and acute worsening of CKD were the most common indications for performing the kidney biopsy.
There are significant functional and structural changes, which naturally occur in the kidney with biological aging. These include decrease in cortical volume with compensatory medullary volume increase and reduction in the number of viable functioning podocytes, leading to glomerular obsolescence affecting the whole-kidney GFR and albumin permeability. The microanatomical changes seen in the kidney are mainly glomerulosclerosis (focal/global), tubular atrophy, interstitial fibrosis, and arteriosclerosis. Functionally, there is an annual decline in the urinary creatinine clearance of 0.75 ml/min.[7] Therefore, interpretation of kidney biopsy of all the compartments of the kidney in the older subpopulation, which includes glomeruli, tubules, interstitium, and blood vessels, the age-related changes should be kept in mind, while making a histological diagnosis.
In our series, there was male predominance, especially those with MN, IgAN, and HBV-GN. These results are partially in concordance with some studies, while other studies reported that there is a slight female predominance or almost equal number of male and female patients in the very elderly patients (over 80 years old). The reason for the gender differences in the two groups may be largely attributed to their greater life expectancy in very elderly women.[4]
NS (with an overall frequency of 27%), either primary or secondary, was the most common indication for kidney biopsy in our study. MN was the leading cause of NS. Many studies conducted in older adult patients (age over 65 years) have shown that Idiopathic Membranous Nephropathy was the most common histopathological diagnosis, followed by amyloidosis and Minimal Change Disease.[4891011] The reasons for this difference may be due to racial and regional disparities. On the other hand, several studies have reported relatively high prevalence of focal segmental glomerulosclerosis (FSGS) in nephrotic patients over 65 years old,[4] while FSGS (6.78%) was only the fourth common histological pattern in our patients with NS.
This subpopulation is more vulnerable to AKI because of the anatomical changes in the kidney with age and due to numerous factors that act as renal stressors such as dehydration, hypotension, postsurgery, nephrotoxic medications, infections, contrast medium exposure, arterial embolic event, and obstructive uropathy.[12] Thus, it is important to identify the possible etiology of AKI early by different means including kidney biopsy. AKI was the third most frequent indication for biopsy in our study accounting for 19.53% of all biopsies performed. This is in accordance with most other studies. However, a recent study suggested that AKI was the leading indication for kidney biopsy in older patients over 80 years.[4] These differences may be due to the discrepancies of ages in the studies. In our study, the most common diagnosis in patients with AKI was acute interstitial nephritis (AIN), followed by ATN. Tubulointerstitial injury might be partly due to drug-induced tubulointerstitial nephritis. Various medications, including nonsteroidal anti-inflammatory drugs, antibiotics, chemotherapeutic medications, and herbal medicines, are still the predominant causes of drug-induced tubulointerstitial nephritis. The usage of herbal medicines is popular in India,[13] which may explain partly the high frequency of AIN in patients with AKI in our study.
There are various clinical manifestations of kidney diseases in older adults, especially in nephritic syndrome and AKI. There are some limitations to diagnosis, treatment, and judgment of prognosis in the kidney diseases by clinical manifestations and laboratory findings alone. Nair et al.[14] reported that in 40% of the patients who underwent kidney biopsy, the diagnosed renal condition was potentially amenable to targeted intervention. It is necessary to perform kidney biopsy in nephritic syndrome and AKI, especially in older patients. The therapeutic schedule should be determined after histopathological diagnosis. Of note, even in patients where the biopsy diagnosis does not directly modify the decision-making of treatment, the histopathological findings offers prognostic information and can also eliminate potentially harmful empiric therapies. Bearing in mind that performing biopsies in this subpopulation is not associated with increased risk for complications, we believe that kidney biopsy is a valuable diagnostic tool that offers the appropriate diagnosis in a clinical setting that maximizes the potential benefit.
Our study has several limitations. First, the retrospective design restricts the amount of data that can be gathered from the medical records of the patients. Second, selection bias might exist since the referral patients in this study were not from the population screened for proteinuria or microscopic hematuria. Therefore, our results need to be confirmed in larger prospective cohort studies.
Conclusion
Kidney biopsy is safe and can provide valuable information for the prognosis and management of diseases in the older subpopulation of patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- India Demographics Profile. 2016. Available from: http://www.indexmundi.com/india/demographics_profile.html
- [Google Scholar]
- What do we know about chronic kidney disease in India: First report of the Indian CKD registry. BMC Nephrol. 2012;13:10.
- [Google Scholar]
- Safety of kidney biopsy in elderly: A prospective study. Int Urol Nephrol. 2006;38:815-20.
- [Google Scholar]
- Benefit of kidney transplantation beyond 70 years of age. Nephrol Dial Transplant. 2010;25:1680-7.
- [Google Scholar]
- Renal diseases in the elderly underwent to percutaneous biopsy of native kidneys. J Bras Nefrol. 2010;32:379-85.
- [Google Scholar]
- Structural and functional changes with the aging kidney. Adv Chronic Kidney Dis. 2016;23:19-28.
- [Google Scholar]
- The renal histopathology spectrum of elderly patients with kidney diseases: A study of 430 patients in a single Chinese center. Medicine (Baltimore). 2014;93:e226.
- [Google Scholar]
- Renal biopsy in very elderly patients: Data from the Spanish registry of glomerulonephritis. Am J Nephrol. 2012;35:230-7.
- [Google Scholar]
- Renal histology in the elderly: Indications and outcomes. J Nephrol. 2012;25:240-4.
- [Google Scholar]
- Revival, modernization and integration of Indian traditional herbal medicine in clinical practice: Importance, challenges and future. J Tradit Complement Med. 2017;7:234-44.
- [Google Scholar]




