

Translate this page into:
Knock Knock
Corresponding Author: Dr. Jasmine Sethi, Department of Nephrology, Post Graduate Institute of Medical Education and Research Chandigarh - 160 012, India. E-mail: jasmine227021@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sethi J, Subramani V. Knock Knock. Indian J Nephrol 2024;34:90. doi: 10.4103/ijn.ijn_429_23
We present a 15-year-old boy who presented with walking difficulty, frequent falls, leg pains, and inward bowing of both knees [Figure 1a] that started 3 years back and, on evaluation, was detected to have renal dysfunction. However, the patient did not seek medical attention then and presented with nausea, vomiting, and worsening of knee deformity. Laboratory evaluation revealed anemia (hemoglobin of 8 gm/dl), serum creatinine of 7.5 mg/dl, serum calcium of 7.5 mg/dl, serum phosphorus of 6.5 mg/dl, alkaline phosphatase of 900 IU/L, serum 25(OH) D of 15ng/ml (25-80), and intact parathyroid hormone level of 450 pg/ml. Ultrasonography revealed bilateral ectopic kidneys with loss of cortico-medullary differentiation. X-ray of thighs showed severe osteopenia and inward bowing of femur [Figure 1b]. A diagnosis of genu valgum (knock knees) and renal osteodystrophy secondary to end-stage kidney disease (ESKD) due to CAKUT was made. The patient was initiated on hemodialysis along with active and elemental vitamin D supplementation, calcium-based phosphate binder, and erythropoietin and advised for renal transplantation. Other manifestations of renal rickets including rachitic rosary, wrist widening, pigeon chest deformity, pot belly, kyphoscoliosis, frontal bossing, and Harrison sulcus groove, were not seen. Most common cause of renal rickets is renal tubular acidosis, followed by azotemic rickets (i.e. ROD in ESKD).1 Factors contributing to renal osteodystrophy in ESKD include chronic metabolic acidosis, reduced formation of 1,25(OH)2 D, and secondary hyperparathyroidism.1 Treatment of genu valgum includes braces for moderate deformity and surgical correction for severe deformity.2
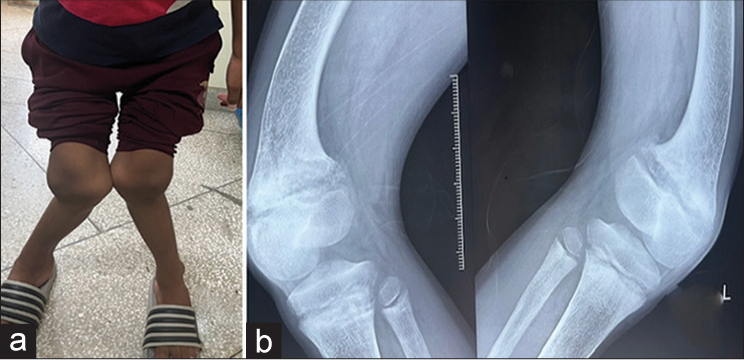
- (a) Patient photograph showing bilateral knock knees (genu valgus) deformity. (b) X-ray anteroposterior at thigh showing bowing of both femur in inward direction at knee.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Renal rickets-practical approach. Indian J Endocrinol Metab. 2013;17(Suppl 1):S35-44.
- [CrossRef] [PubMed] [Google Scholar]
- Correction of severe knees valgus deformities in a patient with renal osteodystrophy. J Am Acad Orthop Surg Glob Res Rev. 2022;6:e22.00113.
- [CrossRef] [PubMed] [Google Scholar]




