

Translate this page into:
Laparoscopic versus Open Surgery Catheter Placement in Peritoneal Dialysis Patients: A Meta-Analysis of Outcomes
Address for correspondence: Dr. Guled Abdijalil, Department of Nephrology, Shaoxing People's Hospital (Shaoxing Hospital Zhejiang University School of Medicine), Shaoxing, Zhejiang 312 000, China. E-mail: guledabdijalil@gmail.com
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
The peritoneal dialysis catheter (PDC) can be placed either through the laparoscopic technique, percutaneous technique, or surgical procedures. The utilization of these PDC placement procedures is based on the successful placement and reduced risk of development of complications. The main objective of this study was to compare the complications associated with the laparoscopic technique to those linked to open surgery during PDC placement.
Methods:
The literature for this review was obtained from the PubMed and Google Scholar databases. The literature search was limited to studies published in the period between 1998 and 2019. The meta-analysis was done using Stata Version 12.
Results:
The results showed a significant difference in catheter malfunction rates between the laparoscopic and open surgery groups (relative risk [RR] = 0.58; 95% confidence interval [CI]: 0.42–0.8, P = 0.031). There was no statistically significant difference in dialysate leakage (RR = 0.77; 95% CI: 0.51–1.17, P = 0.116), peritonitis (RR = 0.8; 95% CI: 0.6–1.06, P = 0.349), and exit-site infection (RR = 0.84; 95% CI: 0.65–1.09, P = 0.834) between two groups.
Conclusion:
In conclusion, the laparoscopic PDC placement procedure was superior to open surgery with regard to catheter malfunction.
Keywords
CAPD catheter insertion
laparoscopy-assisted PDC insertion
PDC insertion by open surgery
peritoneal dialysis catheter insertion

Introduction
Peritoneal dialysis (PD) is one of the accepted alternative treatment methods for end-stage renal disease (ESRD). However, some of the challenges associated with this treatment method include catheter-related infections, leakage of dialysate, and outflow obstruction, among others.[1] Since the introduction of the PD in 1976, increased use of the treatment method has been reported by patients. In the period between 2009 and 2013, for instance, there was a 68% increase in the use of PD among ESRD patients.[2] The increased acceptance of the treatment procedure was attributed to the improved quality of life among patients, the improved catheter survival rates after the first year of dialysis initiation, and good protection of residual renal functioning.[3]
The placement of the peritoneal dialysis catheter (PDC) can be done through an open surgical method, laparoscopic procedure, percutaneous fluoroscopic procedure, or peritoneoscopic implantation.[4] Among the PDC procedures, the open surgical method is commonly used though constrained by high risks of complications among ESRD patients.[5] In recent years, the laparoscopic procedure has been recommended because it is less invasive and has good visibility during catheter placement.[1] Some studies have, therefore, documented the high efficacy of the laparoscopic catheter insertion technique as compared with open surgery.[6] On the other hand, some researchers report that the laparoscopic technique cannot avert the complications of PD.[17]
Amid the contradicting information, no studies have extensively and exhaustively compared the open surgery and laparoscopic PDC placement procedures. Furthermore, the most recent meta-analysis studies have not incorporated the current clinical studies.[8] ESRD continues to contribute significantly to the global burden of disease with an annual increasing rate of 20,000 cases.[910] This study, thus, aimed at comparing the laparoscopic and open surgery catheter placement procedures with regard to catheter-related complications.
Materials and Methods
Search strategy
A comprehensive and systematic literature search was conducted in PubMed and Google Scholar for studies focusing on the comparison between laparoscopic and open surgery catheter placement procedures in PD. The following keywords were used in the search: peritoneal dialysis, open surgery, laparoscopic, catheter placement, and ESRD.
Study selection
The inclusion criteria incorporated studies that were randomized controlled trials, cohort studies, or historical studies. It also included studies that measured PDC placement complications, that is, catheter malfunctioning, dialysate leakages, peritonitis, and exit-site infections. Additionally, only the most recent clinical studies were considered (1998–2019). Studies that were excluded were case reports, letters, and studies with unavailable data. Also, practical guides/manuals, non-English studies, and pediatric studies were excluded from the study. Two independent authors reviewed all the articles obtained in the initial search against the inclusion criteria. Disagreements among the reviewers were resolved through consensus.
Data abstraction
Out of the 50 potential studies, 35 were eliminated due to duplication, unavailability of data, focusing on pediatric studies, being noncomparative studies, and having been written in a non-English language [Figure 1]. The data were abstracted using a standard form that captured the number of patients, demographic characteristics, study design, and PDC placement-related outcomes.
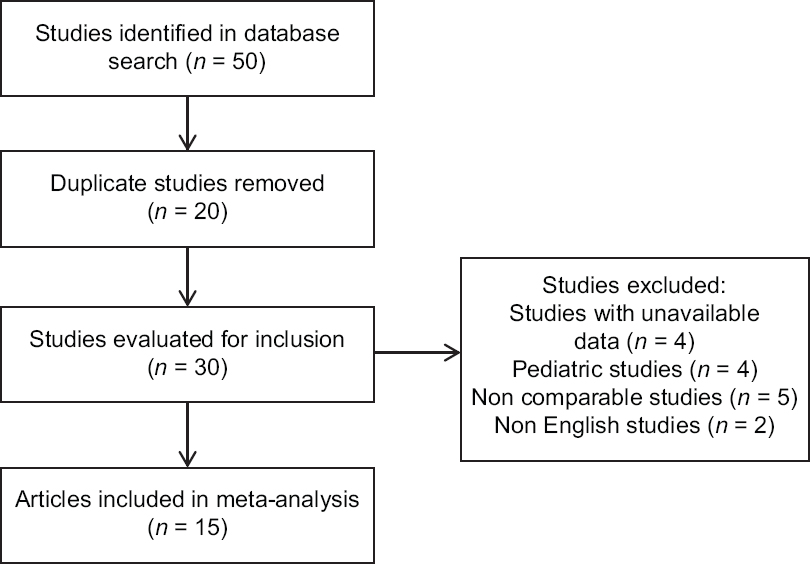
- Selection strategy for studies to be included in the meta-analysis
Statistical analysis
Statistical analysis was conducted using Stata Version 12 (Stata Corporation, College Station, Texas, USA). Meta-analysis was done to compare the key outcomes of interest (dialysate leakage, catheter malfunction, peritonitis, and exit-site infection) between the open surgery and laparoscopic groups. Forest plots were employed to show the between-study variations in effect sizes. Publication bias was assessed using funnel plots. Additionally, small study effects were investigated using Harbord's regression-based test for small study effects. The heterogeneity across the studies was evaluated using the Q statistic and I2 index. Statistical analysis was done at the 95% confidence interval.
Results
The studies included in the meta-analysis followed 4,819 patients. The patients included in the study were adults aged 51.5 ± 33.5 years. The study period for the incorporated studies was from 1998 to 2019 as shown in Table 1.
| Study | Country | Year of publication | Study design | Study period | Number of patients | Age (years) | Comparison | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Tuncer et al.[11] | Turkey | 2003 | Prospective, nonrandomized | March 1998-October 2001 | 42 | 46.9±8.8 | Laparoscopic omental fixation vs. open surgical placement | Complications |
| Soontrapornchai and Simapatanapong[12] | Thailand | 2005 | Prospective, nonrandomized | May 1999-May 2001 | 102 | 57.5±19.1 | Open and laparoscopic secure placement | complications |
| Jwo et al.[1] | China | 2008 | Prospective, randomized | December 2002-October 2006 | 77 | 54.4±16.5 | Open surgery with laparoscopic assisted placement | Positive findings of complications |
| Wright et al.[13] | UK | 1999 | Prospective, randomized | 45 | 49.3±20.2 | Laparoscopic and open peritoneal dialysis | Complications of catheter insertion | |
| Prabhakar et al.[14] | USA | 2019 | Retrospective, nonrandomized | May 2005-March 2018 | 173 | 58.3±1.1 | Laparoscopic and open CAPD placement | Complications (infection, malposition, and malfunction) |
| Atapour et al.[15] | Iran | 2011 | Randomized clinical trial | 2009-2010 | 61 | 55.1±17.2 | Outcome of open surgical procedure and PDC insertion using laparoscopic needle | Complications |
| Cox et al.[16] | USA | 2016 | Retrospective, nonrandomized | 2005-2012 | 3,134 | 59.4±24.0 | Laparoscopic vs. open peritoneal dialysis | Surgical outcomes for PDC placement |
| van Laanen et al.[17] | Netherlands | 2018 | Randomized controlled trial | March 2010-March 2016 | 90 | 63.6±21.3 | Open vs. laparoscopic placement | Reasons for failure and clinical successes |
| Bircan and Kulah[18] | Turkey | 2016 | Prospective, nonrandomized | 2007-2014 | 69 | 63.1±21.1 | Open vs. laparoscopic preperitoneal tunneling | Catheter-related complications |
| Gadallah et al.[19] | USA | 1999 | Prospective, cohort | October 1992-October 1995 | 148 | 46.4±4.5 | Peritoneoscopic vs. surgical placement | Complications and causes of termination of study monitoring |
| Tsimoyiannis et al.[20] | Greece | 2000 | Prospective, randomized | 50 | 60±17 | Laparoscopic placement of the Tenckhoff catheter | Operative variables | |
| Gajjar et al.[21] | USA | 2007 | Retrospective, nonrandomized | 75 | 55.7±32.2 | Laparoscopic vs. traditional placement techniques | Immediate function and complications | |
| Crabtree and Fishman[22] | USA | 2005 | Prospective, cohort | 1992-2002 | 341 | 52.3±16.5 | Basic and advanced laparoscopic vs. open dissection | Clinical details of PDC placement |
| Batey et al.[6] | Kentucky, USA | 2002 | Retrospective, cohort | January 2000-March 2001 | 26 | 45.5±26.5 | Mini laparoscopic-assisted vs. open surgical method | Operative and postoperative data |
| Draganic et al.[23] | Australia | 1998 | Retrospective, cohort | 60 | 50.5±32.5 | Laparoscopy vs. laparotomy | Perioperative complications | |
| Eklund et al.[24] | Finland | 1998 | Retrospective, cohort | June 1994-March 1997 | 102 | 51.1±1.1 | Peritoneoscopic vs. surgical | Catheter- related complications |
| Sun et al.[25] | New Zealand | 2016 | Retrospective, cohort | August 2009-July 2013 | 224 | 55.2±16.4 | Peritoneoscopic vs. surgical | Perioperative outcomes |
CAPD=Continuous ambulatory peritoneal dialysis; PDC=peritoneal dialysis catheter
Based on the meta-analysis, there was no statistically significant difference in dialysate leakages between the laparoscopic and open surgery groups (relative risk [RR] = 0.77; 95% confidence interval [CI]: 0.51–1.17, P = 0.116) [Figure 2]. There was a significant difference in catheter malfunction between the laparoscopic and open surgery groups (RR = 0.58; 95% CI: 0.42–0.80, P = 0.031) [Figure 3]. Comparison of peritonitis between the laparoscopic and open surgery groups showed that neither of the procedures had inferior incidences of peritonitis (RR = 0.8; 95% CI: 0.6–1.06, P = 0.349) [Figure 4]. There was no significant difference in the exit-site infection between the laparoscopic and open surgery groups (RR = 0.84; 95% CI: 0.65–1.09, P = 0.834) [Figure 5].
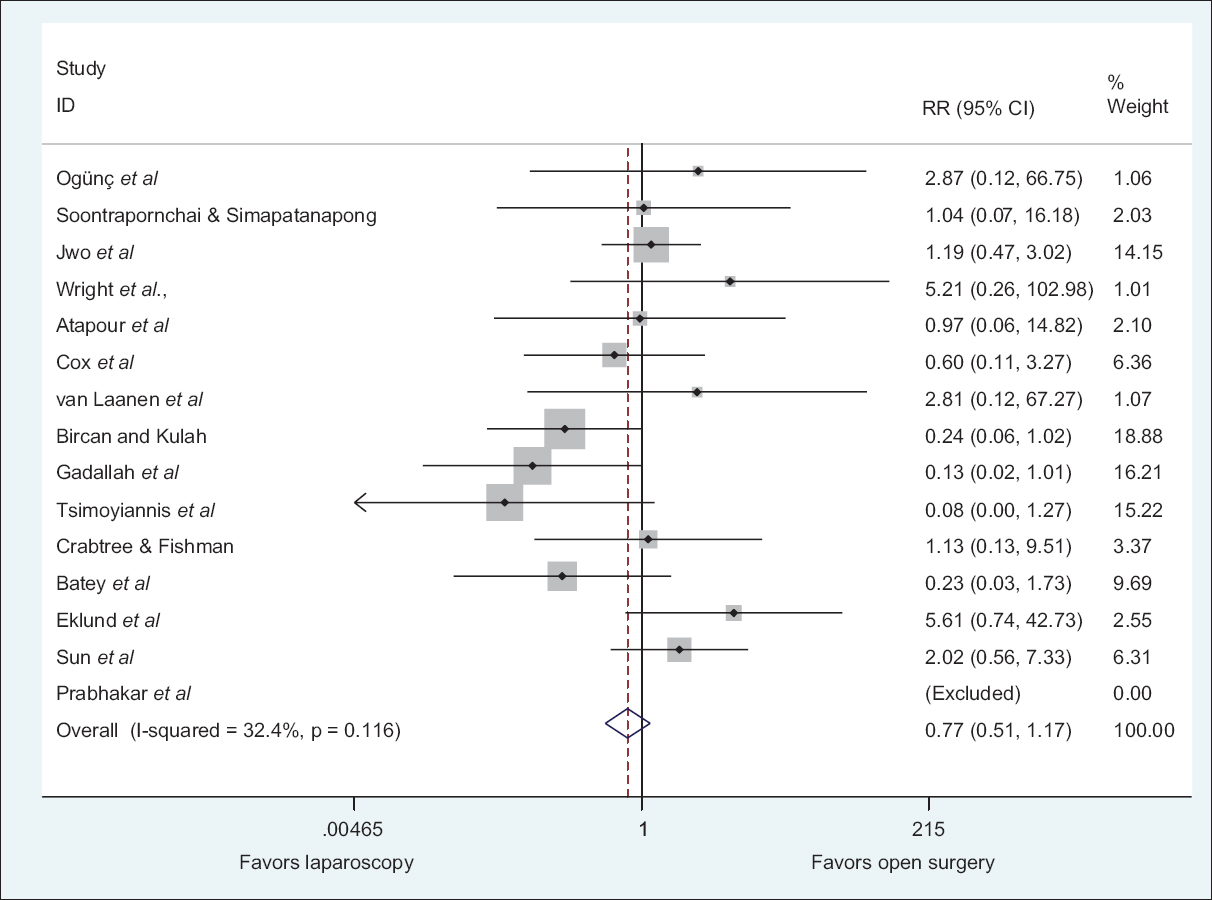
- Relative ratio of dialysate leakages between laparoscopic and open-surgery PDC placement technique

- Relative ratio of catheter malfunction between laparoscopic and open surgery PDC placement techniques
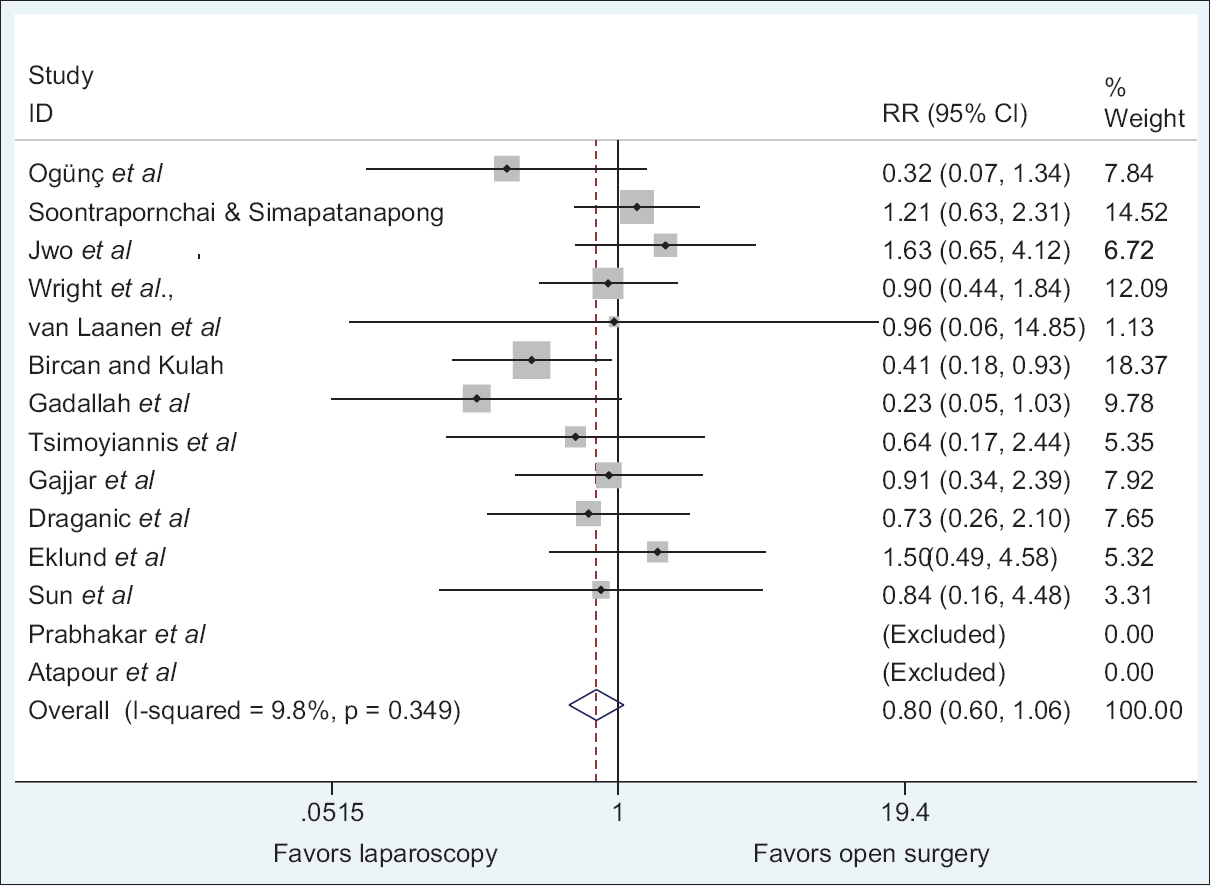
- Relative ratio of peritonitis between laparoscopic and open surgery PDC placement techniques
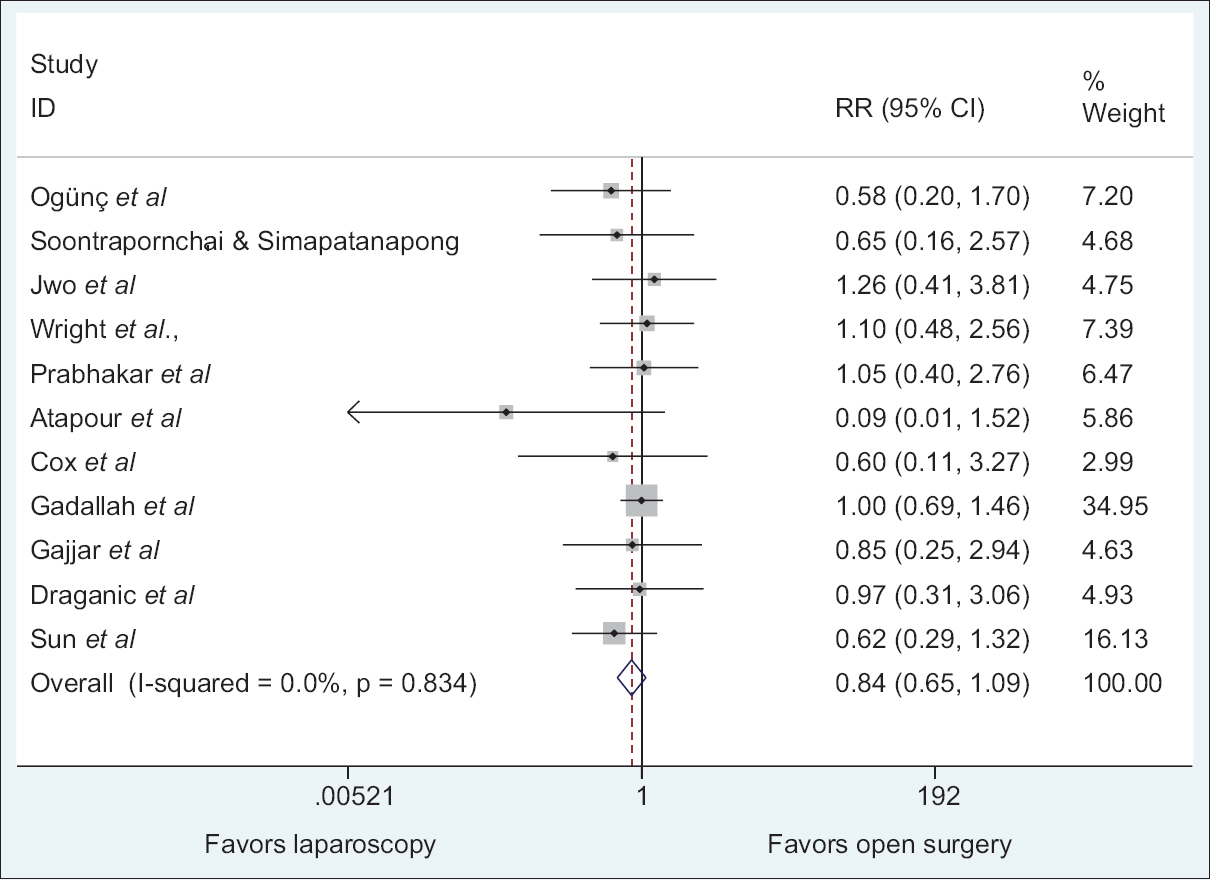
- Relative ratio of exit-site infection between laparoscopic and open surgery PDC placement techniques
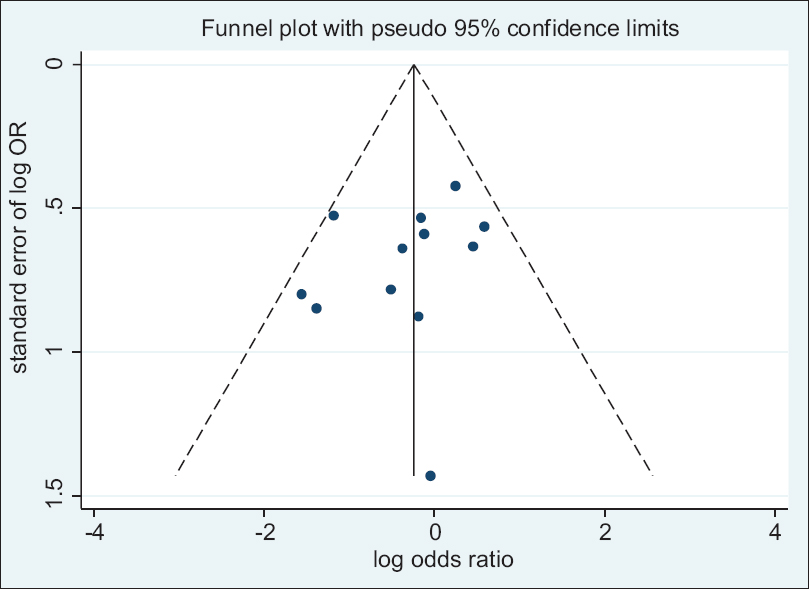
Funnel plots of studies included in the meta-analysis reporting on the occurrence of dialysate leakage, catheter malfunction, peritonitis, and exit-site infection between the laparoscopic and open surgery groups are shown in [Figures 6789]. All funnel plots were symmetrical leading to the conclusion that there was no publication bias. The risk of bias was assessed using the Harbord test as shown in [Tables 2345]. Based on the Harbord regression test, the meta-analysis was not significantly affected by small studies at P < 0.05. Therefore, the meta-analysis could be affected by other factors and not small study effects.

- Funnel plot from all studies comparing dialysate leakage between laparoscopic and open surgery PDC placement techniques

- Funnel plot from all studies comparing catheter malfunction between laparoscopic and open surgery PDC placement techniques
- Funnel plot from all studies comparing peritonitis between laparoscopic and open surgery PDC placement techniques
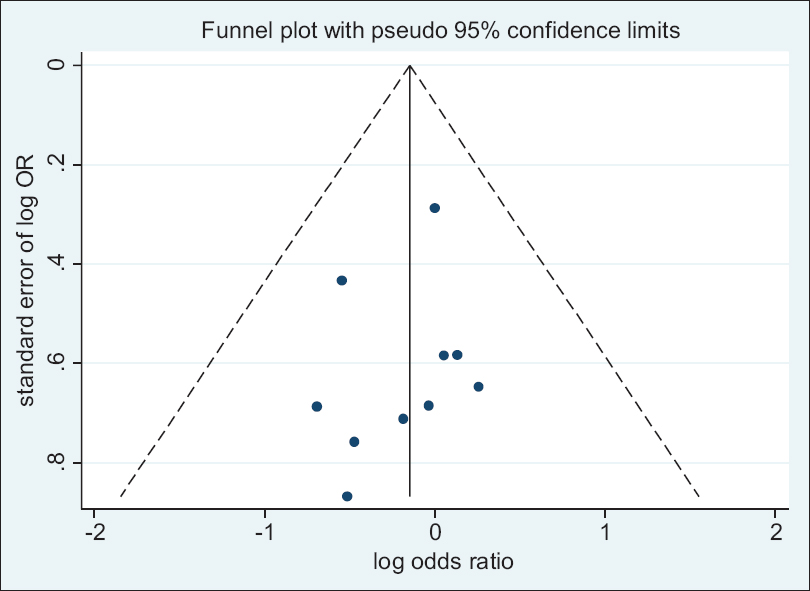
- Funnel plot from all studies comparing exit site infection between laparoscopic and open surgery PDC placement techniques
| Z/sqrt (V) | Coefficient. | Standard Error | t | P>t | 95% Confidence Interval |
|---|---|---|---|---|---|
| Sqrt (V) | −1.24 | 0.9392929 | −1.32 | 0.210 | −3.289221-0.803866 |
| Bias | 1.179963 | 1.094247 | 1.08 | 0.302 | −1.204196-3.564121 |
Test of H0: no small-study effects; P=0.302
| Z/sqrt (V) | Coefficient | Standard Error | t | P>t | 95% Confidence Interval |
|---|---|---|---|---|---|
| Sqrt (V) | −1.35 | 0.9195935 | −1.47 | 0.168 | −3.354368-0.652876 |
| Bias | 1.083912 | 1.333848 | 0.81 | 0.432 | −1.822292-3.990117 |
Test of H0: no small-study effects; P=0.432
| Z/sqrt (V) | Coefficient | Standard Error | t | P>t | 95% Confidence Interval |
|---|---|---|---|---|---|
| Sqrt (V) | 0.05 | 0.771228 | 0.07 | 0.946 | −1.665277-1.77153 |
| Bias | −0.5625115 | 1.290941 | −0.44 | 0.672 | −3.438908-2.313885 |
Test of H0: no small-study effects; P=0.672
| Z/sqrt (V) | Coefficient | Standard Error | t | P>t | 95% Conf. Interval |
|---|---|---|---|---|---|
| Sqrt (V) | 0.24 | 0.3787949 | 0.63 | 0.543 | −0.6175528-1.096234 |
| Bias | −0.9076283 | 0.6999336 | −1.30 | 0.227 | −2.490988-0.6757315 |
Test of H0: no small-study effects; P=0.227
Discussion
The success of PD is measured by the reduction of catheter-related complications. Catheter-related complications may result in technical failures that may reduce catheter survival and may consequently warrant hemodialysis.[26]
The results of this meta-analysis show that there was no statistically significant difference in dialysate leakages between the laparoscopic and open surgery PDC placement. The results of this study were similar to other meta-analysis that reported no significant difference in dialysate leakages between the laparoscopic and open surgery groups.[2728] A number of articles have been published that are concurrent with the findings of the meta-analysis. For instance, a prospective randomized study conducted by Jwo et al.[1] reported no significant difference in dialysate leakage between the laparoscopic and open surgery groups. Similarly, a review done by Crabtree and Fishman[22] revealed no significant differences in the incidences of dialysate leakage between the open surgery and laparoscopic groups.[22] It is worth noting, however, that dialysate leakage is influenced by other factors such as the time when PD was started. Beginning PD immediately after insertion increases the risk of leakage due to inadequate healing of the peritoneum. Additionally, the number of cuffs in a catheter has been documented to influence the occurrence of leaks, especially for the laparoscopic procedure.[28]
The results of the meta-analysis are in agreement with other meta-analyses that concluded that there was a significant difference in catheter malfunction between the laparoscopic and open surgery groups.[28] Similarly, other studies have reported the laparoscopic procedure as a superior catheter placement procedure with lower incidences of catheter malfunction compared with open surgery. For instance, the study by Crabtree and Fishman,[22] which had the highest weight (19.64%), reported higher incidences (17.5%) in the open surgery group compared with the laparoscopic group (0.5%).[1] However, based on a study conducted in the United States, there was no significant difference in the incidences of catheter malfunction between the laparoscopic and open surgery groups.[19] The inconsistency among the studies could be attributed to the differences in the catheters used in different studies.[28] For instance, studies have reported that the use of coiled catheters tends to reduce incidences of catheter malfunction.[29] Additionally, the size of the studies may confound the results of the meta-analysis.
Peritonitis remains a big impediment to the application of PD and a contributor to patients going back to hemodialysis.[30] Based on the results of the meta-analysis, there was no significant difference in peritonitis between the laparoscopic and the open surgery groups (P = 0.349). Similarly, another meta-analysis showed that neither the laparoscopic nor the open surgery PDC placement was superior to the other in terms of peritonitis.[27] The results of this study are also consistent with another meta-analysis that recorded no statistically significant difference in peritonitis between the laparoscopic and open surgery groups.[31] It is worth noting that the results of the meta-analysis could be potentially influenced by factors such as the application of perioperative antibiotics, which has been reported to significantly reduce the risk of the early development of peritonitis.[32] Additionally, studies have documented that there is still no consensus on the type of antibiotics to use to prevent the occurrence of peritonitis as well as when the antibiotics should be administered.[28]
Our meta-analysis suggests that there is no significant difference in exit-site infection between the laparoscopic and open surgery PDC placement (P = 0.834). Based on a study that had the highest weight (34.95%), the incidence of exit-site infection among the open surgery and laparoscopic groups was not significantly different.[19] Furthermore, the results of this study were in agreement with a previous meta-analysis that reported no statistically significant difference in exit-site infection between the patients subjected to a laparoscopic procedure and an open surgery PDC placement.[8] Additionally, based on a meta-analysis done in 2010, there was no difference in the exit-site infection between the two PDC placement procedures.[31] The potential confounding factor of occurrence of exit-site infection in the open surgery and laparoscopic groups is the time when PD was started after the insertion of a catheter. Some studies recommend the immediate start of PD after catheter insertion,[20] other studies recommend a waiting period of 3 to 5 days,[33] whereas some authors suggest a waiting period of 2 weeks.[122122]
The limitation of the study is that six of the 17 studies included in the meta-analysis were nonrandomized. The nonrandomized studies could have contributed to the bias due to uncaptured differences between the groups. Furthermore, the estimates generated were not adjusted, and hence some confounding factors may have affected negatively on the study. Nevertheless, despite the limitations, the meta-analysis provides meaningful information regarding complications associated with laparoscopic and open surgery PDC placement procedures.
Conclusion
The present study shows that there was a statistically significant difference in catheter malfunction between the laparoscopic and open surgery groups. There were, however, no statistically significant differences in dialysate leakage, peritonitis, and exit-site infection between the laparoscopic and open surgery PDC placement procedures.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Prospective randomized study for comparison of open surgery with laparoscopic-assisted placement of tenckhoff peritoneal dialysis catheter-A single center experience and literature... prospective randomized study for comparison of open surgery with lapar. J Surg Res. 2008;159:489-96.
- [Google Scholar]
- Who shouldn't get a percutaneous PD catheter ? Improving clinical outcomes with optimal patient selection and percutaneous techniques for peritoneal dialysis .014.
- [Google Scholar]
- Relative survival of peritoneal dialysis and haemodialysis patients: Effect of cohort and mode of dialysis initiation. PLoS One. 2014;9:1-10.
- [Google Scholar]
- A comparative analysis of percutaneous and open surgical techniques for peritoneal catheter placement. Perit Dial Int. 2012;32:628-35.
- [Google Scholar]
- Surgical complications of Tenckhoff catheters used in continuous ambulatory peritoneal dialysis. Singapore Med J. 2006;47:707-11.
- [Google Scholar]
- Mini-laparoscopy-assisted placement of Tenckhoff catheters : An improved technique to facilitate peritoneal dialysis. J Endourol. 2002;16:681-4.
- [Google Scholar]
- Laparoscopic internal fixation is a viable alternative option for continuous ambulatory peritoneal dialysis catheter insertion. J Korean Surg Soc. 2012;83:381-7.
- [Google Scholar]
- The survival and complication rates of laparoscopic versus open catheter placement in peritoneal dialysis patients: A meta-analysis. Surg Laparosc Endosc Percutan Tech. 2015;25:440-3.
- [Google Scholar]
- Clinical epidemiology of infectious disease among patients with chronic kidney disease. Clin Exp Nephrol. 2019;23:437-47.
- [Google Scholar]
- Global trends in diabetes complications: A review of current evidence. Diabetologia. 2019;62:3-16.
- [Google Scholar]
- Laparoscopic omental fixation technique vs open surgical placement of peritoneal dialysis catheters. Surg Endosc. 2003;17:1749-55.
- [Google Scholar]
- Comparison of open and laparoscopic secure placement of peritoneal dialysis catheters. Surg Endosc. 2005;19:137-9.
- [Google Scholar]
- Randomized prospective comparison of laparoscopic and open peritoneal dialysis catheter insertion. Perit Dial Int. 1999;19:372-5.
- [Google Scholar]
- Outcomes of laparoscopic and open CAPD catheter placement: A single-center experience. Surg Open Sci. 2019;1:20-4.
- [Google Scholar]
- Comparing the outcomes of open surgical procedure and percutaneously peritoneal dialysis catheter (PDC) insertion using laparoscopic needle: A two month follow-up study. J Res Med Sci Off J Isfahan Univ Med Sci. 2011;16:463-8.
- [Google Scholar]
- Laparoscopic versus open peritoneal dialysis catheter placement. Surg Endosc. 2016;30:899-905.
- [Google Scholar]
- Randomized controlled trial comparing open versus laparoscopic placement of a peritoneal dialysis catheter and outcomes: The CAPD I trial. Perit Dial Int. 2018;38:104-12.
- [Google Scholar]
- Effects of a novel peritoneal dialysis: The open versus laparoscopic preperitoneal tunneling technique. Ther Apher Dial. 2016;20:66-72.
- [Google Scholar]
- Peritoneoscopic versus surgical placement of peritoneal dialysis catheters: A prospective randomized study on outcome. Am J Kidney Dis. 1999;33:118-22.
- [Google Scholar]
- Laparoscopic placement of the Tenckhoff catheter for dialvsis peritoneal. Surg Laparosc Endosc Percutan Tech. 2000;10:6-9.
- [Google Scholar]
- Peritoneal dialysis catheters: Laparoscopic versus traditional placement techniques and outcomes. Am J Surg. 2007;194:872-6.
- [Google Scholar]
- A laparoscopic method for optimal peritoneal dialysis access. Am Surg. 2005;71:135-43.
- [Google Scholar]
- Comparative experience of a simple technique for laparoscopic chronic ambulatory peritoneal dialysis catheter placement. Aust N Z J Surg. 1998;68:735-9.
- [Google Scholar]
- Peritoneal dialysis access: A comparison of peritoneoscopic and surgical insertion techniques. Scand J Urol. 1998;32:405-8.
- [Google Scholar]
- Comparison of peritoneal dialysis catheter insertion techniques: Peritoneoscopic, radiological and laparoscopic: A single-centre study. Nephrology. 2016;21:416-22.
- [Google Scholar]
- Laparoscopic placement of Tenckhoff catheters for peritoneal dialysis: A safe, effective, and reproducible procedure. Perit Dial Int. 2008;28:170-3.
- [Google Scholar]
- Laparoscopic versus open catheter placement in peritoneal dialysis patients: A systematic review and meta-analysis. BMC Nephrol. 2012;13:69.
- [Google Scholar]
- Laparoscopic versus open peritoneal dialysis catheter insertion: A meta-analysis. PLoS One. 2013;8:e56531.
- [Google Scholar]
- The curled catheter: Dependable device for percutaneous peritoneal access. Perit Dial Int. 1990;10:231-5.
- [Google Scholar]
- Percutaneous versus surgical insertion of PD catheters in dialysis patients: A meta-analysis. J Vasc Access. 2015;16:498-505.
- [Google Scholar]
- Catheter type, placement and insertion techniques for preventing peritonitis in peritoneal dialysis patients. Cochrane Database Syst Rev 2004:CD004680.
- [CrossRef] [Google Scholar]
- Antimicrobial agents to prevent peritonitis in peritoneal dialysis: A systematic review of randomized controlled trials. Am J Kidney Dis. 2004;44:591-603.
- [Google Scholar]
- Original article comparative experience of a simple technique for laparoscopic chronic ambulatory peritoneal dialysis catheter placement. Aust N Z J Surg. 1998;68:735-9.
- [Google Scholar]




