

Translate this page into:
Late Onset Post-Biopsy Native Kidney Arteriovenous Fistula with Aneurysm in a Renal Transplant Recipient
Corresponding author: Deepesh B Kenwar, Department of Renal Transplant Surgery, Post Graduate Institute of Medical Education and Research, Chandigarh, India. E-mail: deepesh.doc@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gysley BBJW, Bamaniya BB, Kenwar DB, Sethi J, Prabhakar N, Tirkey A. Late Onset Post Biopsy Native Kidney Arteriovenous Fistula with Aneurysm in a Renal Transplant Recipient. Indian J Nephrol. doi: 10.25259/IJN_280_2024
Abstract
Although percutaneous renal biopsy is an essential tool for the diagnosis of renal lesions and parenchymal diseases, this procedure is often associated with a number of complications, of which arteriovenous fistula (AVF) is an important one. We report a case of native kidney post-biopsy AVF in a renal transplant recipient that became symptomatic 20 years later and was successfully managed with native kidney nephrectomy. Our case reveals not only an AVF but also an aneurysm that was asymptomatic for over 2 decades.
Keywords
Renal arteriovenous fistula
Native kidney biopsy
Renal transplant recipient

Introduction
Percutaneous kidney biopsy is a safe procedure, although complications such as renal arteriovenous fistulas (AVF) can occur. Renal biopsy is the most common cause of acquired renal AVFs. Renal AVF occurs when some arteries and veins communicate at the renal hilum or renal parenchyma. In general, post-renal biopsy AVFs do not require any intervention, and they resolve spontaneously in majority of cases.1 Most of these major complications present within 24 hours of biopsy (60% within 4 hours of biopsy). Serious complications like renal AVF are rarely reported beyond 24 hours.2 We report an unusual case of delayed onset native kidney post-biopsy AVF in a renal transplant recipient that was successfully managed with native kidney nephrectomy.
Case Report
A middle aged man in his fifth decade was admitted with complaints of intractable intermittent, severe left loin pain for 15 days duration. In the background, the patient was detected with end stage kidney disease (ESKD) and underwent biopsy of native left kidney in the year 2006 (17 years prior to index presentation). The biopsy was uneventful (no gross hematuria or hematoma was noted), and was reported as IgA nephropathy. Subsequently, the patient underwent HLA compatible live related renal allograft transplant with his brother as the donor. The patient had been stable with good graft function (serum creatinine 0.6 mg/dl) on triple maintenance immunosuppression up to this point. He presented with intractable left loin pain for 2 weeks duration. He denied any history of hematuria, vomiting, dysuria, fever, chills, graft site pain, syncopal attacks, or blood transfusion. Investigations revealed hemoglobin of 11.2 gm/dl, serum creatinine of 1.2 mg/dl, and urine microscopy showed 3 RBC/HPF. Platelet count, coagulogram, urine culture, blood cultures, and serum procalcitonin were within normal limits. Sonography revealed a round, well-defined hypoechoic lesion along the lower pole of the left kidney showing color flow with arterial waveform on Doppler images. CT angiography revealed a saccular contrast-filled outpouching (4 × 2.8 × 3.1 cm) arising from the tortuous left renal artery along the lower pole. Drainage into the left renal vein was seen which was dilated and showed early opacification on arterial phase images. Findings were consistent with AVF with a saccular arterial aneurysm [Figures 1 and 2a]. No perinephric collection was seen. Both native kidneys showed reduced size with irregular outline. Transplanted kidney was seen in the right hemipelvis with normal parenchymal enhancement and no focal lesion. The patient was initially planned for angioembolization of the AV fistula; however, in view of the large size, the procedure was abandoned. The patient was taken for laparoscopic nephrectomy of the left-sided native kidney. Intraoperative findings revealed shrunken and hardened left kidney with fullness visualized over the lower part of the hilum extending toward the lower pole [Figure 2b]. Left renal vein was engorged and multiple perihilar venous collaterals were visualized. The patient was fine 1 week post-operation with stable hemoglobin and was discharged.
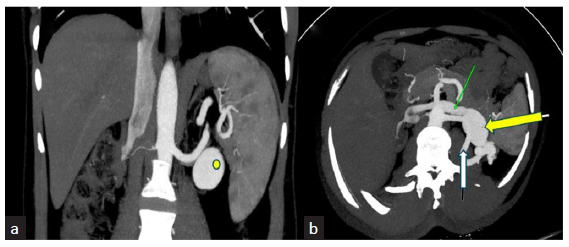
- Contrast CT abdomen (a) (coronal) and (b) (axial) images of arterial phase CT of abdomen showing a saccular contrast filled outpouching (yellow dot/arrow) arising from the left renal artery with drainage into left renal vein (green arrow in b). Also seen is the left renal arteriovenous fistula (white arrow in b).
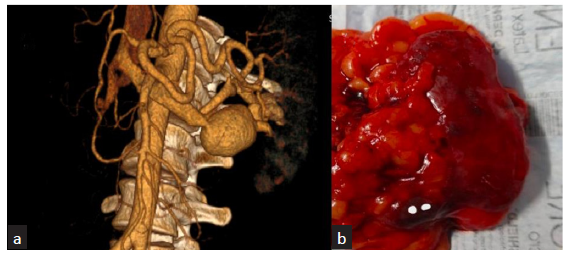
- (a) 3D Reconstructed Angiographic image showing large aneurysmal sac draining in to left main renal vein. (b) Post Nephrectomy specimen showing left kidney with lower pole aneurysmal sac due to arteriovenous fistula.
Discussion
With the almost universal use of automatic biopsy needles and real-time ultrasound guidance, the incidence of renal AVF is reduced to below 0.1%.3 Risk factors for renal AVFs post-biopsy include hypertension, large (14G) biopsy needle, renal fibrosis, nonultrasound-guided biopsy, and nephrosclerosis.4 It could be possible in our patient that the fistula was initially small and asymptomatic, but minor trauma or heparin administration in dialysis led to an increase in the size of the renal AVF. Recently, Oyama et al. published a case of renal AVF that was detected 2 years after native kidney biopsy.5 There are reports of renal AVF detected as late as 10 years after kidney biopsy.6 To our knowledge, this is the first case of native kidney AVF detected after 20 years in a renal transplant recipient thus making our case unique.
CT angiography is the investigation of choice in cases with a strong clinical or sonographic suspicion of a vascular complication post-biopsy, and helps delineate the exact cause (AVF/pseudoaneurysm), its location, extent, and associated rupture or hematoma. Our case reveals not only an AVF but also an aneurysm that was asymptomatic for over 2 decades. Although slow growing, renal artery pseudoaneurysms following renal biopsy have been reported previously in literature this rare finding of a slow growing AVF with a concomitant feeder artery aneurysm contributes to the uniqueness of our case. A proper follow-up ultrasound examination of the kidney soon after renal biopsy and 6 months later is recommended for early detection of nonresolving AVFs to prevent further complications.7
Conclusion
We experienced a case of renal arteriovenous fistulas (RAVF), which was discovered with refractory flank pain 17 years after renal biopsy. Even if complications such as RAVFs are not observed early after renal biopsy, considering the possibility of delayed RAVF, regular follow-up with US after renal biopsy even in asymptomatic cases could be important.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
References
- Renal arteriovenous fistula after renal biopsy: A case report and literature review. J Vasc Bras. 2019;18:e20180112.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Risk factors and timing of native kidney biopsy complications. Nephron Extra. 2014;4:42-9.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Arteriovenous fistulae after renal biopsy: Diagnosis and outcomes using Doppler ultrasound assessment. BMC Nephrol. 2017;18:365.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Childhood asymptomatic renal arteriovenous fistula 5 years after renal biopsy. Pediatr Int. 2018;60:601-2.
- [CrossRef] [PubMed] [Google Scholar]
- Renal arteriovenous fistula discovered ∼2 years after renal biopsy: A case report. Clin Case Rep. 2023;11:e7538.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Two cases of incidentally detected renal arteriovenous fistula over ten years after renal biopsy. Nihon Jinzo Gakkai Shi. 2016;58:33-7.
- [PubMed] [Google Scholar]
- Arteriovenous fistulae after renal biopsy: Diagnosis and outcomes using doppler ultrasound assessment. BMC Nephrol. 2017;18:365.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




