

Translate this page into:
Nontuberculous Mycobacterial Graft Pyelonephritis in a Post-Renal Transplant Recipient
Corresponding author: Faheem Nazir Qanoongo, Department of Nephrology, Gauhati Medical College and Hospital, Gauhati, Assam, India. Email: faheemnazir0011@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sharma M, Qanoongo FN, Doley PK, Pegu G, Pegu M. Nontuberculous Mycobacterial Graft Pyelonephritis in a Post-Renal Transplant Recipient. Indian J Nephrol. doi: 10.25259/IJN_326_2024
Abstract
Nontuberculous mycobacterial (NTM) infections pose significant challenges in renal transplant recipients. We present a case of Mycobacterium chelonae graft pyelonephritis in a 19-year-old female post-ABO incompatible renal transplantation. The patient presented with a subcutaneous abscess over the graft site, which revealed pyelonephritis with perinephric collection. Persistent symptoms prompted the identification of M. chelonae. Management included tailored antimicrobial therapy and surgical debridement, resulting in full recovery and improved graft function. This case highlights the importance of considering NTM infections in transplant recipients with atypical presentations and emphasizes the need for species identification and susceptibility testing to guide effective treatment.
Keywords
NTM infections
Renal transplant
Mycobacterium chelonae
Graft pyelonephritis
Antimicrobial therapy

Introduction
Nontuberculous mycobacterial (NTM) infections, though uncommon, can lead to severe complications in renal transplant recipients.1 These infections present diagnostic and therapeutic challenges due to their diverse clinical manifestations, inherent antimicrobial resistance, and complex drug interactions.2 We report a rare case of Mycobacterium chelonae graft pyelonephritis in a renal transplant recipient, highlighting the diagnostic and therapeutic challenges encountered.
Case Report
A 19-year-old female underwent a living-related ABO incompatible renal transplant (A to O) on March 23, 2023, with her mother as the donor. The patient had been diagnosed with Immunoglobulin A (IgA) nephropathy in September 2022 and progressed to end-stage renal disease by October 2022, requiring hemodialysis. Prior to transplantation, she underwent desensitization, reducing her anti-A titer from 1:128 to 1:2.
The patient received induction therapy with basiliximab, and the transplant procedure was uneventful. Her initial posttransplant course was favorable, and she was discharged on POD 10 with serum creatinine of 0.8. However, two months posttransplant, she developed posttransplant diabetes mellitus and experienced episodes of urinary tract infections caused by Klebsiella pneumoniae.
In November 2023, the patient presented with pain and swelling at the graft site. Ultrasound revealed graft pyelonephritis with a perinephric collection extending from the intraparenchymal space to the subcutaneous tissue, resulting in abscess formation. She was empirically started on intravenous piperacillin-tazobactam and linezolid for three weeks. Mycophenolate mofetil (MMF) was withheld, while tacrolimus (TAC) and prednisolone were continued.
Incision and drainage of the abscess was performed, followed by secondary suturing. Pus analysis revealed acid-fast bacilli (AFB), but the Cartridge-Based Nucleic Acid Amplification Test (CBNAAT) for Mycobacterium tuberculosis complex was negative. Suspecting an NTM infection, the patient was empirically started on ethambutol, isoniazid, and azithromycin, adjusted for creatinine clearance.
Despite initial improvement, the swelling recurred [Figure 1a], necessitating another incision and drainage procedure [Figure 1b]. In January 2024, persistent pus discharge was observed, and culture reports confirmed the presence of NTM. Doxycycline and Faropenem were added to the treatment regimen. A repeat ultrasound was performed, which indicated minimal perinephric collection. She was transitioned to a triple immunosuppressant therapy comprising MMF, TAC, and Wysolone after withholding MMF for four weeks. The sample was sent for NTM species identification and antibiotic sensitivity testing.
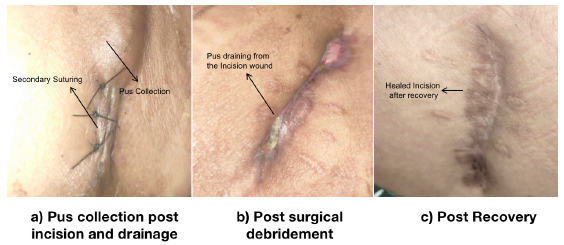
- (a-c) Stages of surgical wound healing in a case of mycobacterial infection.
In February 2024, ongoing pus discharge necessitated further intervention. The wound was reopened and deep sloughing of necrotic tissue was performed. Clarithromycin and levofloxacin were added to the treatment regimen, while faropenem and azithromycin were discontinued.
In March 2024, the causative organism was identified as M. chelonae, with susceptibility testing revealing sensitivity to linezolid, clarithromycin, amikacin, and tobramycin. The final treatment regimen was modified to include linezolid and clarithromycin for 3 months while discontinuing resistant antimicrobials based on the susceptibility testing results. Linezolid was planned to continue for at least six months after clinical improvement, with the possibility of extending up to 12 months based on the patient’s response.
By April 2024, the patient had fully recovered, with no active discharge or signs of inflammation around the wound site [Figure 1c] and significant improvement in graft function. Laboratory findings of the case are presented in Table 1.
| 20/11/2023 | 30/11/2023 | 07/12/2023 | 28/04/2024 | |
|---|---|---|---|---|
| Hemoglobin | 6.7 g/dL | 7.2 g/dL | 10.8 | |
| Total leukocyte count | 26.1 × 109/L | 9.1 × 109/L | 8.0 × 109/L | |
| Random blood sugar | 77 mg/dL | 88 mg/dL | ||
| Urea | 64 mg/dL | 29 mg/dL | 46 mg/dL | 36 |
| Creatinine | 2.44 mg/dL | 1.64 mg/dL | 1.58 mg/dL | 1.34 |
| C-Reactive protein | 81 mg/L | 35 mg/L | 28 mg/L | 8 |
| Urine analysis | Albumin trace, RBC (‒), Pus Cells 6–7/HPF | |||
| Tacrolimus (Co) | 4.52 ng/mL | |||
| Urine culture | Sterile | |||
| Gram staining | No microorganism | |||
| AFB staining | AFB detected | |||
| Culture for NTM | No growth (within five days) | |||
| GeneXpert for MTB | Not detected | |||
| Fungal staining | No fungal elements |
AFB: acid-fast bacilli; NTM: nontuberculous mycobacteria; MTB: mycobacterium tuberculosis; RBC: red blood cells; HPF: high power field
The exact source of the M. chelonae infection was not identified; however, it was speculated that the patient might have been exposed to the organism through nosocomial and environmental sources, such as water or soil, during the posttransplant period.
Discussion
NTM infections are rare but with potentially devastating complications in renal transplant recipients, with reported incidences ranging from 0.16% to 0.38%.3 M. chelonae, a rapidly growing NTM species, has been associated with various clinical presentations, including skin and soft tissue infections, pulmonary disease, and disseminated infections.4
The diagnosis of NTM infections can be challenging due to nonspecific clinical manifestations and limitations of conventional microbiological techniques.5 In this case, the initial pus analysis revealed AFB, but CBNAAT was negative for M. tuberculosis. NTM was identified only after further evaluation of persistent pus discharge and a six-week culture, highlighting the importance of maintaining a high index of suspicion in transplant recipients with atypical presentations.
Management of NTM infections requires a combination of antimicrobial therapy and surgical intervention when necessary.6 In this case, the patient was initially started on a modified antimycobacterial regimen, which was later tailored based on species identification and susceptibility testing. Surgical debridement of necrotic tissue and antiseptic dressing were also performed to facilitate healing.
The management of M. chelonae infections in transplant recipients requires prolonged antimicrobial therapy, typically lasting at least six months after clinical improvement. The source of infection in such cases is often challenging to identify, but may be related to environmental exposure or nosocomial infections.
Choosing appropriate antimicrobial agents for M. chelonae infections is particularly challenging due to the organism’s inherent resistance to many antibiotics and potential drug interactions.
Conclusion
This case highlights the importance of considering NTM infections in renal transplant recipients, particularly in cases of nonresolving or atypical infections. Early diagnosis, species identification, susceptibility testing, and appropriate management, including tailored antimicrobial therapy and surgical intervention when necessary, are crucial for better graft and patient survival outcomes.
Conflicts of interest
There are no conflicts of interest.
References
- An official ATS/IDSA statement: Diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175:367-416.
- [CrossRef] [PubMed] [Google Scholar]
- Risk factors for nontuberculous mycobacterial infections in solid organ transplant recipients: A case-control study. Transpl Infect Dis. 2014;16:76-83.
- [CrossRef] [PubMed] [Google Scholar]
- Nontuberculous mycobacterial infection in hematopoietic stem cell and solid organ transplant recipients. Clin Infect Dis. 2004;38:1428-39.
- [CrossRef] [PubMed] [Google Scholar]
- Mycobacterium chelonae cutaneous infection: A challenge for an internist. Eur J Case Rep Intern Med. 2021;8:003013.
- [CrossRef] [PubMed] [Google Scholar]
- Understanding nontuberculous mycobacterial lung disease: It’s been a long time coming. F1000Res. 2016;5:2797.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- A case of cutaneous mycobacterium chelonae abscessus infection in a renal transplant patient. J Cutan Med Surg. 2001;5:28-32.
- [CrossRef] [PubMed] [Google Scholar]




