

Translate this page into:
Osteitis Fibrosa Cystica
Address for correspondence: Dr. Sourabh Agstam, VMMC, Safderjanj Hospital, New Delhi, India. E-mail: sourabhagstam@gmail.com
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 19-year-old boy, an active sportsperson was hospitalized 2 months back for evaluation of fracture of right arm associated with trivial trauma while playing cricket. The patient was referred to our tertiary care centre for further evaluation of an abnormal radiograph of right humerus done at a community hospital.
On further enquiry, he recollected history of having fracture of right humerus at the same spot 4 years back that had healed within a 4 weeks period. On examination, he had spindle shaped deformities of phalanges of both hands and the patient attributed these abnormalities to repeated insignificant trauma to hands and fingers while playing cricket especially on trying to catch the cricket ball. The rest of the examination was unremarkable. The skeletal survey picked up multiple cystic lesions in the humerus [Figure 1a and b], carpals, metacarpals, phalanges of both upper limbs [Figure 2]. The X-ray of bilateral feet revealed cystic lesions on 5thmetatarsal on both sides [Figure 3]. Laboratory evaluation revealed normal blood counts, electrolytes, liver function tests, and urinalysis. Patient had azotemia (serum urea = 81 mg/dl, serum creatinine = 4.9 mg/dl) with normal serum total calcium = 9.2 mg/dl (normal8.0--10.4), serum phosphate = 3.7 mg/dl (normal 2.5--4.5), and elevated serum total alkaline phosphatase = 591U/L (normal 25-100 U/l). Serum intact PTH level was 1742 pg/ml (Normal10--65 pg/ml) and 25-hydroxy vitamin D 8 ng/ml (Normal20--40 ng/ml). 99 m Technetium MIBG (metaiodobenzylguanidine) parathyroid scan showed delayed washout of the tracer suggestive of right lower parathyroid adenoma. A diagnosis of chronic kidney disease with tertiary hyperparathyroidism was entertained and the patient was planned for minimal invasive parathyroid adenomectomy and subsequent renal replacement therapy. This case was missed for 4 years after the first fracture and therefore serves to make clinicians aware of the condition.
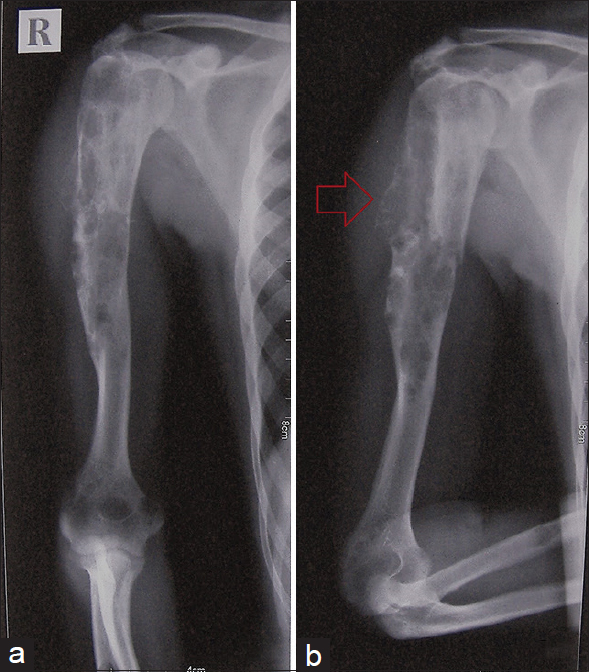
- (a and b) Multiple cystic lesions in right humerus and prominence of pathological fracture on elbow flexion (Red arrow)

- Generalized osteolytic lesions, subperiosteal resorption and multiple cystic lesions in phalanges, metacarpals, carpal and radius bone of bilateral upper limb

- Cystic lesions on 5th toe and metatarsal of both feet (Red arrow).
Osteitis fibrosa cystica is also known as brown tumor, cystica generalisata, or Recklinghausen's disease of bone developing due to the accumulation of hemosiderin within the vascularized fibrous tissue. Overt radiological signs of hyperparathyroidism associated skeletal disease like osteitis fibrosa cystica are commonly seen with parathyroid carcinoma.[12]
Declaration of patient consent
The author certifies that he has obtained appropriate patient consent. Patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that his name and initials will not be published, and due efforts will be made to conceal his identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Clinical review 122: Parathyroid carcinoma. J Clin Endocrinol Metab. 2001;86:485-93.
- [Google Scholar]
- Brown Tumor of Hyperparathyroidism: Bony Lesions.Diagnostic Surgical Pathology of the Head and Neck (2nd ed). Philadelphia: Sanders; 2009.




