

Translate this page into:
Post-Transplantation Hypervolemia and Renal Allograft Outcomes
Corresponding author: Macaulay Onuigbo, Department of Medicine, The Robert Larner, M.D. College of Medicine, University of Vermont, Burlington, Vermont, United States. E-mail: macaulay.onuigbo@uvmhealth.org
-
Received: ,
Accepted: ,
How to cite this article: Onuigbo M. Post-Transplantation Hypervolemia and Renal Allograft Outcomes. Indian J Nephrol. doi: 10.25259/IJN_48_2025
Dear Editor,
We eagerly read the article ‘Extracellular Fluid Volume and Mortality after Kidney Transplantation’ in the journal ‘Kidney360’. The report was a bicentric prospective cohort of 2057 kidney transplant recipients who underwent glomerular filtration rate (GFR) measurement (mGFR) three months after transplantation.1 This report demonstrated the independent association between elevated extracellular fluid volume (ECV) (measured three months post-transplantation) and increased mortality and decreased mGFR (measured 12 months post-transplantation) without graft loss.1
In 2024, two patients experienced delayed graft function aggravated by iatrogenic hypervolemia due to peri-operative fluid administration post-transplantation. This was at the University of Vermont Kidney Transplant Program in Burlington VT, USA. We built a case on one patient to support the idea that iatrogenic IVF-induced hypervolemia is responsible for delayed graft function via congestive allograft nephropathy.
A 63-year-old female with end-stage kidney disease from polycystic kidney disease received a deceased donor kidney in mid-August of 2024. The patient had slow graft function, minimal urine output, and increasing hypervolemia, primarily due to IV fluid administration. This continued despite giving IV furosemide (120 mg) and chlorothiazide (500 mg) every six and eight hours [Figure 1].

- Increasingly positive hypervolemia, mostly from IV fluid therapy, despite combination of IV diuretics. IV: Intravenous.
Due to persistent hyperkalemia, hyponatremia, and hyperphosphatemia, she had an urgent three-hour hemodialysis (HD) treatment with ultrafiltration two days post-operation. She did not need any additional HD. Serum creatinine was at 1.52 mg/dL two weeks post-transplantation [Figure 2].
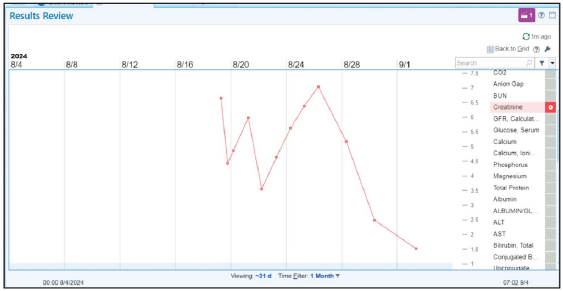
- Serum creatinine trajectory following deceased donor kidney transplantation with delayed graft function and significant improvement in renal allograft function at 2 weeks post-transplantation. BUN: Blood urea nitrogen, GFR: Glomerular filtration rate, ALT: Alanine transaminase, AST: Aspartate transaminase.
Ould Rabah et al. confirmed hypervolemia’s negative impact post-transplantation by investigating ECV’s effect on renal allograft function.1 To our knowledge, these are the first reports on delayed renal allograft function due to congestive nephropathy resulting from iatrogenic peri-operative IVF-induced hypervolemia. In view of this unrecognized syndrome, we advocate for a more nuanced and balanced approach to the perioperative IV fluid use post-transplantation to avoid hypervolemia.
Conflicts of interest
There are no conflicts of interest.
Reference
- Extracellular fluid volume and mortality after kidney transplantation. Kidney360. 2024;5:1902-12.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




