

Translate this page into:
Renal Manifestation in Scrub Typhus during a Major Outbreak in Central Nepal
Address for correspondence: Dr. A. Sedhain, Department of Medicine, Nephrology Unit, Chitwan Medical College, Bharatpur, Chitwan, Nepal. E-mail: arunsedhain@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Renal involvement and acute kidney injury (AKI) are common clinical manifestations seen in scrub typhus, a vector-borne tropical disease. There are no data on renal manifestation in scrub typhus in Nepal. We conducted a prospective study to analyze the incidence, urinary abnormalities, course, severity, outcome, and the predictors of AKI in patients with scrub typhus during a major outbreak in Central Nepal. Total 1398 patients admitted with acute febrile illness were subjected for Scrub Typhus Detect™ Immunoglobulin M (IgM) enzyme-linked immunosorbent assay (ELISA) test, of which 502 (35.90%) patients tested positive and were included in the study. Mean age of the patients was 30.37 ± 18.81 years (range, 1–79 years) with 26.29% in the pediatric age group. Female-to-male ratio was 1.26:1. Mean duration of fever was 6.8 ± 3.1 days. Mean IgM ELISA value for scrub typhus was 2.17 ± 1.70 without difference in AKI and non-AKI groups (2.17 ± 1.76 vs. 2.16 ± 1.62; P = 0.94). Urinary abnormalities were seen in 42.3% of patients. Mean serum creatinine was 1.37 ± 0.69 mg/dl with significant difference in two groups (1.85 ± 0.87 vs. 1.03 ± 0.17; P = 0.003). AKI was seen in 35.8% of patients with majority having Stage 1 AKI (68.3%) followed by Stage 2 (34.1%) and Stage 3 (1.2%). Hemodialysis was required for 3.94% of patients. In 54% of patients, AKI occurred in fifth and sixth day of fever. ICU admission was required for 18.73% of patients and 8.57% required ventilator support. Mortality rate was 1.79%, which was higher among patients with AKI (2.96% vs. 1.0%; P = 0.106). Multivariate analysis revealed that the presence of pneumonia, shock, and acute respiratory distress syndrome predicted the development of AKI.
Keywords
Acute febrile illness
acute kidney injury
albuminuria
hematuria
scrub typhus

Introduction
Scrub typhus is a vector-borne disease caused by the organism Orientia tsutsugamushi. It is transmitted through the bite of larval forms (chiggers) of trombiculid mites.[12] Most common presentation of scrub typhus is nonspecific febrile illness with constitutional symptoms such as fever, rash, myalgias, and headache. Multiorgan dysfunctions involving organs such as kidney, liver, lungs, central nervous system, or with circulatory collapse could be the other modes of presentation in severe form of the disease.
Renal involvement in scrub typhus is a common manifestation, which might range from 10% to 60% with multifactorial etiopathogenetic mechanism.[1] The spectrum of renal involvement might range from subtle urinary abnormalities including albuminuria and active urinary sediments such as cellular casts, pyuria, and hematuria to acute kidney injury (AKI) requiring urgent initiation of renal replacement therapies.
In Nepal, scrub typhus as a cause of acute febrile illness (AFI) was first reported long back in 1981.[3] Another hospital-based study conducted in 2004 found that 3% of cases admitted to the hospital with AFI were found to have scrub typhus.[4] Since then, the disease has been considered to be endemic in different parts of the country, though it did not cause significant problems. Recently published few reports have highlighted the burden of this disease in the country[56] but none of them studied the renal effects of scrub typhus. Hence, this prospective study was carried out in a tertiary level teaching hospital with an aim to find out the incidence, urinary abnormalities, course, severity, outcome, and the predictors of AKI among the patients with scrub typhus.
Subjects and Methods
This was a prospective analytical study conducted from April to December 2016 in the Department of Medicine at Chitwan Medical College Teaching Hospital. The approval from the ethical committee and informed written consent from the patients were taken before the study. Patients admitted with AFI who were tested positive for Scrub Typhus Detect™ IgM ELISA test (titer equal or more than 0.5) were included in the study. Patients who concomitantly had other infections such as dengue, leptospirosis, typhoid fever, brucella, or malaria and patients already diagnosed to have chronic kidney disease were excluded from the study.
Clinical, laboratory, and demographic variables were recorded in all patients. All patients had a detailed clinical history and examination by the specialist physician. A standard set of investigations including complete blood counts, liver function tests, and renal function tests including serum urea, creatinine, and electrolytes were done. Chest radiograph and ultrasound of abdomen and pelvis were performed. Urinary abnormalities as defined by dipstick proteinuria, pyuria, hematuria, and casts as seen on urine microscopy were documented in all patients. AKI was defined as per kidney disease improving global outcome (KDIGO) guideline. Patients were divided into two groups – with or without AKI – and the clinical characteristics and outcomes were compared between AKI and non-AKI groups.
Descriptive and inferential statistical analyses was done using SAS University Studio package. Patient characteristics were summarized using mean and frequency distributions. Data for continuous variables were expressed as mean ± standard deviation using t-test for continuous variables and Chi-square test for categorical variables. Analyses of variation tests were done to test the differences of continuous variables across multiple groups.
Results
Out of 1398 patients with AFI subjected for Scrub Typhus Detect™ IgM ELISA test, 502 (35.90%) patients were tested positive. Mean age of the patients was 30.37 ± 18.81 years with age range between 1 and 79 years. Twenty-six percent of the patients were in pediatric age group. Females comprised 55.98% of the patients with female-to-male ratio of 1.26:1. The baseline characteristics in both groups matched to each other [Table 1].

The majority of the patients (72%) were from the areas largely hit by 7.8 magnitude earthquake in April 2015. Most of them belonged to the rural (32%) and semi-urban (24%) areas of the country.
The first case of scrub typhus during this outbreak was seen in April and majority (97.98%) of the patients were seen between July and November with highest number of patients seen in October.
All patients included in the study had fever. Other clinical presentations in the descending order of frequency were anorexia (55.18%), headache (53.39%), lymphadenopathy (15.73%), jaundice (13.35), eschar (6.57%), neurologic manifestations (6.37%), and cardiac manifestations (4.38%). We did not find any significant differences between two groups of patients in terms of clinical presentations.
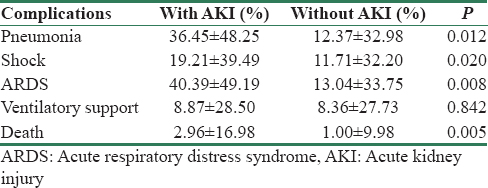
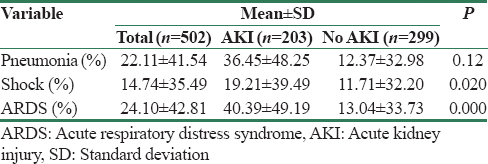
Most common complication seen was acute respiratory distress syndrome (ARDS) followed by pneumonia and shock [Table 2]. Mortality was 1.79%, which was significantly higher in the AKI than in the non-AKI group (2.96% vs. 1.0%; P = 0.005). Factors that predicted mortality were development of shock, presence of AKI at the time of admission, pneumonia, and requirement of ICU care and ventilatory support.
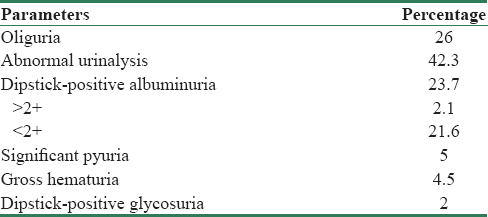
There was no significant difference between AKI and non-AKI group in terms of laboratory parameters [Table 3]. Anemia was seen in 35.28% of patients. Leukocytosis (total leukocyte counts >11,000/mm3) was found in 5.78% of patients without significant differences in AKI and non-AKI groups (4.93% vs. 6.35%; P = 0.501) and thrombocytopenia (platelet count <150,000/mm3) in 66.73% of patients with 66.89% and 66.5% in AKI and non-AKI groups, respectively. Transaminitis was seen in 80.68% of patients with majority having raised AST than ALT (90.63 vs. 86.65%; P = 0.531). Urinary abnormalities were seen in 42.3% of patients [Table 4].
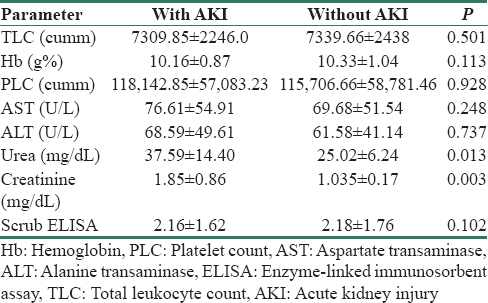
Dyselectrolytemia was seen in 17.67% of patients, most common of which was hyponatremia seen in 9.54% of patients followed by hyperkalemia (6.26%), hypokalemia (1.34%), and hypernatremia (0.53%). Mean serum creatinine was 1.37 ± 0.69 mg/dl with significant higher value in the AKI group (1.85 ± 0.87 vs. 1.03 ± 0.17 mg/dl; P = 0.003). AKI was seen in 35.8% of patients with majority of them having stage 1 AKI (66%) followed by stage 2 (33%) and stage 3 AKI (1%) [Figure 1]. Hemodialysis was required for 3.94% of patients with AKI, the indications of which were anuria and volume overload, severe metabolic acidosis, and persistent hyperkalemia.
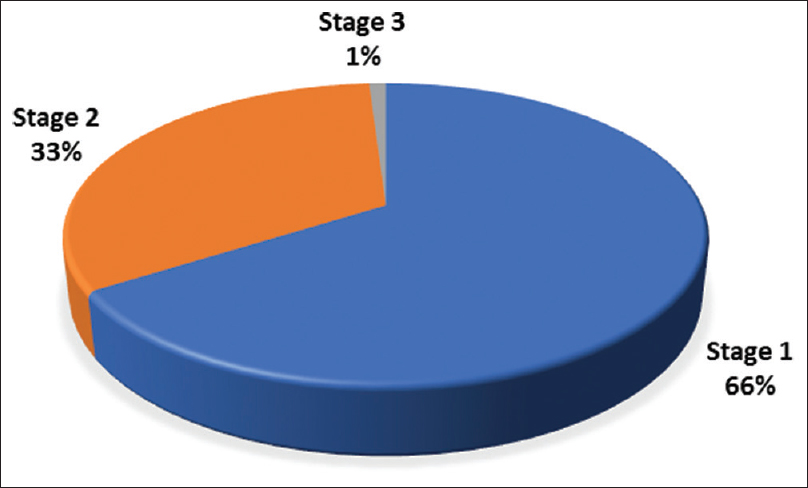
- Stages of acute kidney injury in scrub typhus
Among patients with AKI, 28% of patients were ≤14 years, 65% were between 15 and 59 years, and 7% were more than 60 years of age. The age of the patients was not associated with renal outcome. Among the patients with AKI, 96.06% of patients had complete recovery with mean serum creatinine value of 0.94 mg/dl at the time of discharge, 2.96% died, and 0.98% left the hospital against medical advice. We did not find any correlation between occurrence of AKI and the ELISA titer of scrub typhus [Table 5].
In univariate analysis, there was a significant correlation between different clinical parameters such as pneumonia, ARDS, and shock with the development of AKI [Table 6]. However, none of the laboratory parameters including scrub ELISA titer could predict the AKI development.
The major findings of the study are summarized in [Figure 2].
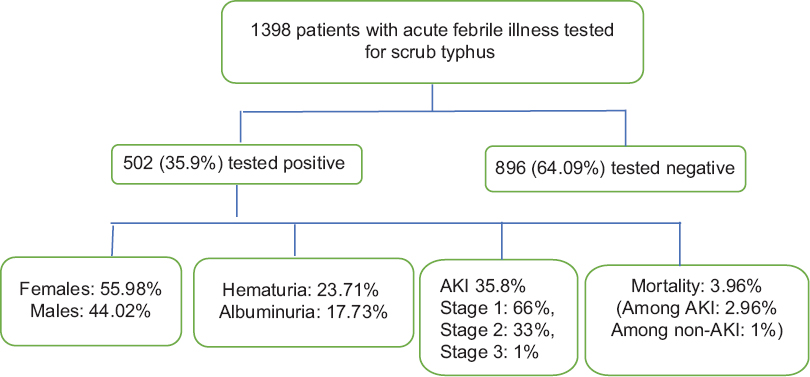
- Flowchart of the results
Discussion
This is the first study to comprehensively describe the clinical presentation, laboratory investigation, pattern of renal involvement, and outcome in a cohort of patients of scrub typhus in Nepal. We have found that scrub typhus was responsible for about 36% of patients presenting with unexplained febrile illness.
Scrub typhus is a mite-borne infectious disease caused by the obligate intracellular Gram-negative bacteria O. tsutsugamushi. It is transmitted by the bite of an infected trombiculid mite larva.[7] The disease was first described from Japan in 1899, and in the initial days, the overall mortality varied from 7% to 9%.[8] In the current days, scrub typhus is endemic to a part of the world known as the “tsutsugamushi triangle.”[9] In Nepal, scrub typhus as a cause of AFI was first detected in 1981 in Eastern part where 10% of study population were found to have antibodies to scrub typhus rickettsiae.[4] In another study, up to 3% of in hospital patients in Central Nepal were found to be infected with the scrub typhus.[7] However, till date, there is not a single study to analyze the renal manifestation of scrub typhus infection. The current outbreak of scrub typhus in Nepal was seen from those areas, which were affected by the 7.8 magnitude earthquake. These outbreaks were thought to be due to people and rodents living in close proximity in temporary shelters after the earthquake.[1011] Majorities of the patients included in our study were from the earthquake-affected areas [Figure 1].
The adult mites have a four-staged lifecycle, namely, egg, larva, nymph, and adult. The larval stage, also known as chigger, is the only stage that can transmit the disease to humans and other vertebrates.[9] The incubation period of scrub typhus in human is around 10–12 days and the clinical manifestation varies from mild febrile illness to severe multiorgan dysfunction syndrome, which may be fatal at times. Apart from the non-specific generalized clinical features,[12] the significant findings of scrub typhus are eschar formation at the site of bite, the prevalence of which is variable ranging from 7% to 80%.[1314] However, eschar is rarely seen in South East Asia and Indian subcontinent.[1516] Lymphadenopathy, usually painful, is a common finding in scrub typhus reported in 13%–18% of patients.[171819] Respiratory distress and encephalitis are the principal causes of death in patients with severe disease.[20] All patients included in this study had fever followed by anorexia, headache, jaundice, and lymphadenopathy. Eschar formation was seen only in 8% of the patients. There was no significant difference between the AKI and non-AKI group in terms of clinical presentation.
Diagnosis of scrub typhus requires a high degree of clinical suspicion, which is confirmed serologically by different laboratory investigations.[21] The cheapest test currently available and used extensively in Indian subcontinent is Weil–Felix test which is highly specific, but lacks sensitivity.[2223] IgM ELISA using the 56 kDa antigen has been widely used, which is easy to perform, gives quick results, and has sensitivity of 84%–86% and a specificity of 98%[2425] and is well validated.[26] On the basis of ELISA titer, the result is interpreted as negative (<0.2), equivocal (0.2–0.5), and positive (>0.5).[24] PCR amplification of the 56-kDa protein gene has been demonstrated to be a reliable method for diagnosing scrub Typhus.[27] However, none of the current diagnostic test is sufficiently practical and technically feasible for use by physicians working in rural areas. A new dipstick test using a dot blot immunoassay format appears to be the best currently available test for diagnosing scrub typhus in rural areas where this disease predominates.[28]
AKI and renal involvement in scrub typhus is believed to be multifactorial in origin. Overall, renal involvement is considered to be a part of multiorgan dysfunction syndrome in patients with severe disease.[2129] Frequently described causes are impaired renal perfusion resulting from shock or hypovolemia or increased vascular permeability, rhabdomyolysis, vasculitis, acute interstitial nephritis, thrombotic microangiopathy secondary to disseminated intravascular coagulation, and acute tubular necrosis due to direct microbial invasion of the renal tubules.[303132] Histopathological findings on renal biopsy show acute tubular necrosis, interstitial nephritis, and mild mesangial glomerulonephritis.[3334] Reported severe clinical manifestations or complications of scrub typhus include meningoencephalitis, myocarditis, pneumonia, ARDS, AKI, GI bleeding, septic shock, and multiorgan failures which may be potentially fatal if there is a delay in diagnosis and treatment.
In our study, urinary abnormalities were seen in 52.94% of patients with proteinuria being the most common presentation (23.71%) followed by hematuria (17.73%), pyuria (5%), gross hematuria (4.5%), and dipstick-positive glycosuria (2%). The incidence of these urinary abnormalities suggests intrinsic renal involvement being the most likely explanation. Urinary abnormalities have been reported in 50%–80% of patients with scrub typhus.[35] Attur et al. in their study from South India reported urinary abnormalities in all patients with AKI.[33] Most common urinary abnormality in their study was proteinuria seen in 28.6% of patients followed by active sediments, granular casts, hematuria, and pyuria.
In this study, 35.8% of the patients developed AKI, which is consistent with findings in other studies where its incidence has been reported ranging from 10% to 60%.[33363738] Most of the patients had Stage 1 and 2 AKI comprising 66% and 33%, respectively, and only 1% of patients had Stage 3 AKI. The only peculiarity of ours in comparison to previous studies was that we defined AKI according to KDIGO guideline, whereas RIFLE criteria were used by others. The identification of the most appropriate tool to define and classify AKI in scrub typhus could be one of the scopes in future studies. In one study from South India, which used RIFLE criteria to define and categorize AKI, renal involvement in scrub typhus was mild with 60% of the patients having RIFLE class risk or injury.[33] In our study, 3.94% of patients with AKI required hemodialysis, which was lower than other studies done in Indian population.[3135]
In our study, the presence of pneumonia, ARDS, and shock predicted the development of AKI. Interestingly, the titer of scrub typhus ELISA did not correlate with the incidence and severity of AKI. In studies from South India in children with AFI, scrub typhus was one of the causes of AKI with thrombocytopenia, requirement of intensive care,[34] and myocarditis[36] being significantly associated with AKI.
Mortality in this study was 1.79%, which was significantly higher in the AKI than in the non-AKI group (2.96% vs. 1.0%; P = 0.005). Higher rate of mortality in AKI patients could be the reflection of underlying severity of disease. Our finding is comparable to other studies, which ranged from 0.79% to 12%.[153439] Vivekanandan et al. in their study from South India reported the mortality of 12.2%.[13] Another Indian study by Kumar et al. found the mortality as high as 16.32% among patients with scrub typhus, which was significantly higher among patients with oliguric AKI. All three patients who had dialysis-dependent AKI expired in that study.[35] Lower mortality in our study was probably due to early diagnosis and initiation of treatment. Delayed presentation, ARDS, and shock have been shown to be the determinants of mortality in previous studies.
There are certain limitations to our study. This was a single-center study done in Central Nepal and might not reflect the national scenario as the outbreak of scrub typhus had been reported from other areas of the country. Second, the diagnosis of scrub typhus was made based on the ELISA test and we excluded patients with equivocal results (ELISA titer between 0.2 and 0.5). Although the ELISA method has a satisfactory sensitivity and specificity, nucleic acid amplification tests would have brought better results. Third, we did not compare the renal manifestation between AFI patients with or without scrub typhus. Another limitation of our study was the use of KDIGO guideline rather than pRIFLE to define and stage AKI in pediatric population. The use of KDIGO criteria could be problematic for smaller pediatric patients, including infants and children with low muscle mass.
Conclusion
Scrub typhus has emerged as an important cause of febrile illness with multisystem involvement in Nepalese context. Renal involvement including the development of AKI is a common systemic manifestation in scrub typhus. We suggest that scrub typhus should be part of the differential diagnosis in patients with AFI and AKI.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Diagnosis and treatment of scrub typhus – The Indian scenario. J Assoc Physicians India. 2010;58:11-2.
- [Google Scholar]
- The etiology of febrile illness in adults presenting to Patan hospital in Kathmandu, Nepal. Am J Trop Med Hyg. 2004;70:670-5.
- [Google Scholar]
- Scrub typhus. 2013. Medicine Update. India: Association of Physicians of India; :19-22. Available from: http://www.apiindia.org/medicine_update_2013/chap06.pdf
- [Google Scholar]
- Clinical presentation of scrub typhus during a major outbreak in central Nepal. Asian J Med Sci. 2017;8(4):27-31.
- [Google Scholar]
- Threat of scrub typhus in post-earthquake Nepal. Journal of Chitwan Medical College. 2016;6(18):1-6.
- [Google Scholar]
- Scrub typhus. In: Beran GW, ed. Handbook of Zoonoses (2nd ed). Florida: CRC Press; 1994. p. :663-8.
- [Google Scholar]
- Leptospirosis in Malaya. I. Sporadic cases among military and civilian personnel. Am J Trop Med Hyg. 1957;6:238-56.
- [Google Scholar]
- Typhoid versus typhus fever in post-earthquake Nepal. Lancet Glob Health. 2016;4:e516-7.
- [Google Scholar]
- Scrub typhus: Clinical, pathologic, and imaging findings. Radiographics. 2007;27:161-72.
- [Google Scholar]
- Distribution of eschars on the body of scrub typhus patients: A prospective study. Am J Trop Med Hyg. 2007;76:806-9.
- [Google Scholar]
- Epidemiologic, clinical and laboratory features of scrub typhus in thirty Thai children. Pediatr Infect Dis J. 2003;22:341-5.
- [Google Scholar]
- Investigation of an outbreak of scrub typhus in the Himalayan region of India. Jpn J Infect Dis. 2005;58:208-10.
- [Google Scholar]
- Scrub typhus in patients reporting with acute febrile illness at a tertiary health care institution in Goa. Indian J Med Res. 2012;136:1020-4.
- [Google Scholar]
- Milder clinical manifestation of scrub typhus in Kinmen, Taiwan. J Formos Med Assoc. 2013;112:201-7.
- [Google Scholar]
- Scrub typhus: Surveillance, clinical profile and diagnostic issues in Shandong, China. Am J Trop Med Hyg. 2012;87:1099-104.
- [Google Scholar]
- Life-threatening scrub typhus in a traveler returning from Thailand. Clin Infect Dis. 1994;18:624-6.
- [Google Scholar]
- Orientia tsutsugamushi (scrub typhus) In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases Vol 1. (7th ed). Philadelphia: Churchill Livingstone, Elsevier; 2009. p. :2529-30.
- [Google Scholar]
- Relevance of Weil-Felix test in diagnosis of scrub typhus in India. J Assoc Physicians India. 2006;54:619-21.
- [Google Scholar]
- Evaluation of tests for serological diagnosis of scrub typhus. Trop Doct. 2006;36:212-3.
- [Google Scholar]
- Diagnostic accuracy of the InBios scrub typhus detect enzyme-linked immunoassay for the detection of IgM antibodies in Northern Thailand. Clin Vaccine Immunol. 2015;23:148-54.
- [Google Scholar]
- Scrub typhus among hospitalised patients with febrile illness in South India: Magnitude and clinical predictors. J Infect. 2006;52:56-60.
- [Google Scholar]
- Detection and characterization of Rickettsia tsutsugamushi (Rickettsiales: Rickettsiaceae) in infected Leptotrombidium (Leptotrombidium) fletcheri chiggers (Acari: Trombiculidae) with the polymerase chain reaction. J Med Entomol. 1994;31:691-9.
- [Google Scholar]
- Scrub typhus. In: Warrel DA, Cox TM, Firth JD, Benj EJ jr, eds. Oxford Textbook of Medicine Vol 1. (4th ed). Oxford: Oxford University Press; 2003. p. :629-31.
- [Google Scholar]
- Scrub typhus (Orientia tsutsugamushi) In: Kliegman RM, Stanton BF, Geme JW 3rd, Schor NF, Behrman RE, eds. Nelson Textbook of Pediatrics (19th ed). Philadelphia: Saunders, Elsevier; 2011. p. :1045-6.
- [Google Scholar]
- A case of acute renal failure, rhabdomyolysis and disseminated intravascular coagulation associated with scrub typhus. Clin Nephrol. 2003;60:59-61.
- [Google Scholar]
- Tsutsugamushi infection-associated acute rhabdomyolysis and acute renal failure. Korean J Intern Med. 2003;18:248-50.
- [Google Scholar]
- Acute renal failure due to acute tubular necrosis caused by direct invasion of Orientia tsutsugamushi. J Clin Microbiol. 2008;46:1548-50.
- [Google Scholar]
- Scrub typhus associated with multiorgan failure: A case report. Scand J Infect Dis. 1997;29:634-35.
- [Google Scholar]
- Scrub typhus is an under-recognized cause of acute febrile illness with acute kidney injury in India. PLoS Negl Trop Dis. 2014;8:e2605.
- [Google Scholar]
- Scrub typhus in children at a tertiary hospital in Southern India: Clinical profile and complications. J Infect Public Health. 2012;5:82-8.
- [Google Scholar]
- Acute kidney injury in tropical acute febrile illness in a tertiary care centre – RIFLE criteria validation. Nephrol Dial Transplant. 2011;26:524-31.
- [Google Scholar]
- Scrub typhus associated acute kidney injury – A study from a tertiary care hospital from Western Himalayan state of India. Ren Fail. 2013;35:1338-43.
- [Google Scholar]
- Scrub typhus: An unrecognized threat in South India – Clinical profile and predictors of mortality. Trop Doct. 2010;40:129-33.
- [Google Scholar]




