

Translate this page into:
The Role of Renal Angiography in Hepatitis B-related Polyarteritis Nodosa
Address for correspondence: Dr. R. Malhotra, 3350 La Jolla Village Drive, 9111H, San Diego, CA 92161-9111, USA. E-mail: r3malhotra@ucsd.edu
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Case
A 45-year-old female presented to our facility with a 3-month history of persistent headache and abdominal pain. She also complained of vertigo, blurred vision, and bilateral eye pain. She had a medical history significant for hypertension, hypothyroidism, and chronic Hepatitis B infection. Physical examination revealed blood pressure of 148/68 mmHg and pulse of 64/min, and diplopia was pronounced when looking to the right. Fundi were normal. Cardiovascular and respiratory system and abdominal examination were unremarkable. Computer tomographic (CT) scan of brain was normal. CT angiography of the head was negative for aneurysm or thrombus. Laboratory work was negative for complement levels, antinuclear antibody, anticardiolipin antibodies, and cryoglobulins. Hemoglobin and plasma biochemistry were normal. Erythrocyte sedimentation rate was elevated with a value of 60 mm/h and C-reactive protein of 15 mg/l. Urine microscopy was normal with no proteinuria. Hepatitis B surface antigen was positive and hepatitis B virus (HBV) DNA as detected by polymerase chain reaction revealed a viral load of more than 318,337 copy/ml. Renal angiogram, performed because of a suspicion of polyarteritis nodosa (PAN), showed multiple microaneurysms in the renal circulation [Figure 1]. The patient was started on steroid and tenofovir therapy with symptomatic improvement.
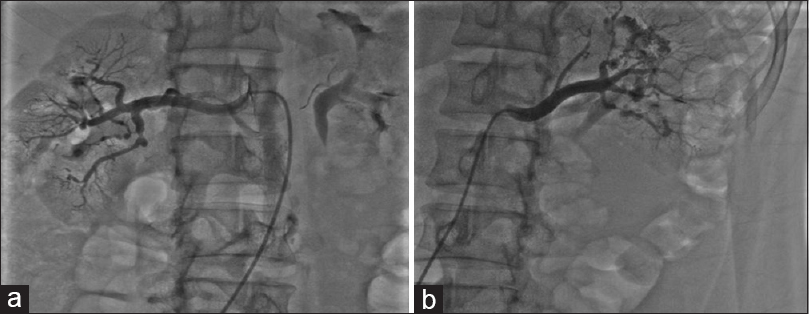
- (a and b) Renal artery aneurysms
Diagnosis
Patient was diagnosed as a case of Hepatitis B-related Polyarteritis Nodosa.
Discussion
PAN is a systemic disease, characterized by panmural necrotizing vasculitis affecting small- and medium-sized arteries. PAN is more common in males between fifth and seventh decade. The etiology of PAN is largely unknown. HBV infection may play an important role in the disease pathogenesis by deposition of HBeAg/anti-HBe immune complexes in vessel walls resulting in focal inflammation.[1] The clinical spectrum of PAN ranges widely from mild forms with fever, malaise, arthralgias or arthritis, skin rash, neuritis to severe form with renal, or gastrointestinal involvement. Kidney is commonly involved in 70%–80% of cases of PAN with clinical manifestations ranging from malignant hypertension, proteinuria, renal insufficiency, or hemorrhage due to microaneurysms. However, occasionally, clinical features may be absent or exceedingly variable and thus making the diagnosis of PAN quite challenging. The tissue biopsy of symptomatic organ may provide definite diagnosis of PAN, but sampling errors and lack of disease specificity limit the value of biopsy. Studies have shown that angiography is a valuable diagnostic tool with a sensitivity of 89% and a specificity of 90% for PAN.[2] The most striking angiographic finding includes appearance of aneurysms, usually microaneurysms, ectasia, or occlusive disease. Spontaneous perinephric hematoma and retroperitoneal hemorrhage may result from a ruptured renal artery aneurysm and can be potentially fatal complication of PAN. Renal angiography should be considered in cases where PAN is suspected despite having stable and normal renal function.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Polyarteritis nodosa and extrahepatic manifestations of HBV infection: The case against autoimmune intervention in pathogenesis. J Autoimmun. 2001;16:269-74.
- [Google Scholar]
- Diagnostic significance of angiographically observed visceral aneurysms with regard to polyarteritis nodosa. Acta Radiol. 1991;32:143-8.
- [Google Scholar]




