

Translate this page into:
Trilateral Reflux in a Child with Renal Transplant

Corresponding author: Akshay Kumar Saxena, Department of Radiodiagnosis and Imaging, Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India. E-mail: fatakshay@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Kotia K, Bhatia A, Sodhi KS, Malik MA, Saxena AK, Trilateral Reflux in a Child with Renal Transplant. Indian J Nephrol. 2024;34:672-3. doi: 10.25259/IJN_105_2024
A 12-year-old boy presented with recurrent urinary tract infections, a follow-up case of renal transplantation following chronic kidney disease (CKD) due to posterior urethral valve (PUV), which was surgically managed by transurethral fulguration previously. The child underwent micturating cystourethrography (MCU) to look for vesicoureteral reflux (VUR). VUR was seen on MCU in bilateral native kidneys. On the right side, reflux of contrast was seen in the ureter and pelvicalyceal system (PCS), which were not dilated, suggestive of grade II VUR [Figure 1]. On the left side, there was reflux of contrast into the ureter and PCS, which were mildly dilated with blunting of forniceal angles and maintained papillary impressions, suggestive of grade III VUR [Figure 1]. In addition, VUR was also seen in the transplanted kidney in the right iliac fossa, with findings suggestive of grade III VUR [Figure 1].
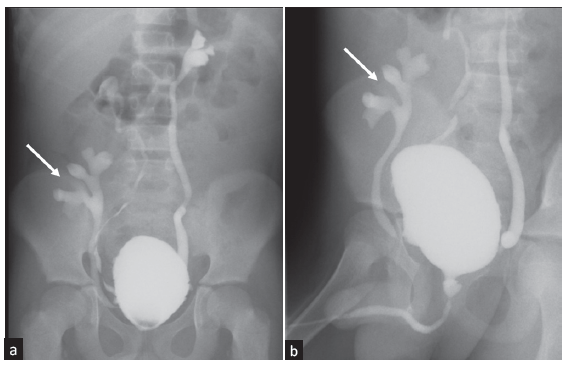
- (a-b) Spot images of micturating cystourethrography show grade II vesicoureteral reflux on the right side and grade III vesicoureteral reflux on the left side. Grade III vesicoureteral reflux is seen in the transplanted kidney in the right iliac fossa (arrows in a and b).
VUR in the native kidneys, especially in cases with significant ureteral dilatation, is identified as a potential risk factor for the occurrence of urinary tract infections (UTIs) in children.1 While the surgical technique of ureteric anastomosis can decrease VUR in transplanted kidneys, the occurrence of VUR, specifically in the transplanted kidney itself, is likely common and generally not problematic in the absence of infection. However, post-transplant acute pyelonephritis (APN) has the potential to harm the transplanted kidney through scarring. Hence, it is crucial to minimize the occurrence of symptomatic UTIs and mitigate their effects on the future function and survival of the kidney allograft.2
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent from the parents.
Conflicts of interest
There are no conflicts of interest.
References
- Vesicoureteral reflux after kidney transplantation in children. Nephrol Dial Transplant. 2000;15:1852-8.
- [CrossRef] [PubMed] [Google Scholar]
- Vesico-ureteric reflux in children and young people undergoing kidney transplantation. Pediatr Nephrol. 2023;38:2987-93.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




