

Translate this page into:
A histopathological outlook on nephrotic syndrome: A pediatric perspective
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
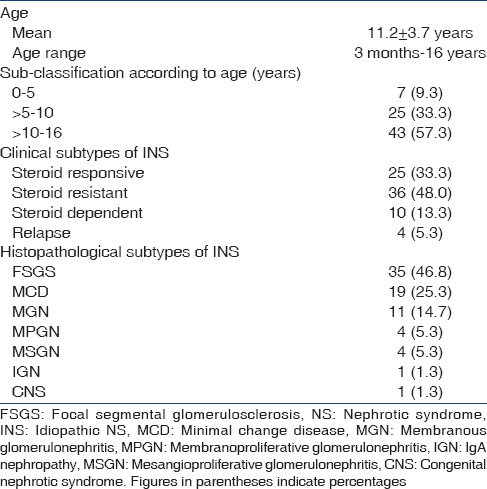
The developing world is observing changing histopathological patterns of idiopathic nephrotic syndrome (INS). However, the true burden of non-minimal change disease (non-MCD) presenting as INS remains unestimated owing to a paucity of data on renal biopsies. Data were collected from January 2006 to June 2014 on 75 children up to 16 years of age who underwent renal biopsies for INS. Mean age at biopsy was 11.2 ± 3.7 years. The male to female ratio was 1.5:1. A total of 25 (33.3%) children were steroid sensitive, 36 (48%) were steroid resistant, 10 (13.3%) were steroid dependent and 4 (5.3%) came with relapse of nephrotic syndrome (NS). Focal segmental glomerulosclerosis (FSGS) was the most common histopathological subtype observed in 35 (46.8%) children followed by membranous glomerulonephritis (MGN) in 11 (14.7%), membranoproliferative glomerulonephritis (MPGN) and mesangioproliferative glomerulonephritis (MSGN) in 4 (5.3%) each and IgA nephropathy in one (1.3%). MCD was the histological lesion in 19 (25.3%) children. The histopathology established FSGS as the main underlying cause of steroid resistant NS. The study highlights the emergence of non-MCD as the common cause of INS in the pediatric population and signifies the importance of renal biopsies in children with INS.
Keywords
Children
focal segmental glomerulosclerosis
minimal change disease
nephrotic syndrome
renal biopsy

Introduction
Nephrotic syndrome (NS) is a common childhood renal disease characterized by a remitting and relapsing pattern;[1] it is a manifestation of different histopathological subtypes;[2] the true incidence of various histopathological subtypes of NS remains unestimated owing to a diversity of criteria for performing renal biopsies in pediatric population.[3] Consequently, the delay in the diagnosis and initiation of management has strong implication on the disease outcome. Histopathological examination of the renal biopsy is fundamental not only in establishing the diagnosis, but also guides treatment and prognosis[4] rendering renal biopsy, the gold standard procedure. Percutaneous renal biopsy has now been established as a safe and low-risk procedure in children of all ages. The advent of an automated biopsy device and real-time ultrasound for percutaneous renal biopsies has enhanced the probability of obtaining adequate tissue for diagnosis and has reduced the complications associated with the procedure.[56] The projected annual incidence of NS is 2–7/100,000 children, affecting mostly those under 6 years of age (1–3). Children continue to experience disease flare-ups for a considerable period of time from onset.[1] One of the earliest studies on histological findings of renal biopsies published in 1970s reported minimal change disease (MCD) as the most common subtype in children with NS.[78] Subsequent data on the incidence of NS have remained unchanged over the past three decades. However, change in the histological patterns is being increasingly observed and reported. Hence, this study aims to identify the recent trends of histopathological patterns of NS from a developing country tertiary care center.
Materials and Methods
A cross-sectional study was conducted at the Histopathology Department of Aga Khan University Hospital on children up to 16 years of age who underwent renal biopsy between January 2006 and June 2014. A total of 128 charts were reviewed; only those children with NS as the indication of renal biopsy were included. Steroid dependence was defined as relapse on withdrawal of steroids and requirement of steroids to maintain the remission. Steroid resistance was defined as the absence of remission despite daily therapy with steroids for 4 weeks. Recurrence of proteinuria in a child previously in remission was referred to as relapse.[9] About 75 children met the criteria; their demographic data, clinical and histopathological subtypes were recorded. All renal biopsy specimens were processed, cut and stained, and evaluated under light microscopy and immunofluorescence technique. Biopsies were stained with h and e and periodic acid Schiff. The Immunofluorescence staining was performed on 4 µm thick cryostat sections obtained from snap-frozen tissue or on paraffin embedded tissue sections. The sections were tested with antibodies and complement components including immunoglobulin G (IgG), IgM, IgA, C3, C1q, and fibrinogen. Biopsies that were either inadequate or suggestive of secondary causes of NS were excluded. Statistical Package for Social Sciences (SPSS) version 19.0 (IBM Corp. San Francisco) was used for statistical analysis. Categorical variables were reported as frequencies and percentages and continuous variables as mean ± standard deviation. For descriptive purposes, data were stratified according to age and were reported in tabulated and graphical form.
Results
A total of 75 children with adequate renal biopsy specimens were included. All children had undergone biopsy for NS. A renal biopsy is not routinely performed at our center if children clinically behave like minimal change NS. However, children with symptoms that make MCD unlikely such as gross hematuria, hypertension, renal insufficiency, or hypocomplementemia are considered for renal biopsy. Patients with steroid sensitive nephrotic syndrome (SSNS) were biopsied when they experienced relapse and decision regarding alternate therapy (cyclosporine, tacrolimus) had to be made. In our study, 45 (60%) children were male, and 30 (40%) were female. The male to female ratio was 1.5:1. The mean age at onset of NS was 11.2 ± 3.7 years. Three subgroups were made according to age to see the distribution of the disease; 0–5 years, 5–10 years and >10 years. The majority of the children were older than 10 years of age [Table 1]. The most common indication for renal biopsy in our children was steroid resistance occurring in 36 (48%) children. About 25 (33.3%) children were steroid sensitive, 10 (13.3%) were steroid dependent and 4 (5.3%) had experienced a relapse [Table 1]. MCD was the histopathological subtype in 19 children (25%); overall, about 75% of children had non-MCD subtype on renal biopsy regardless of age. FSGS was the most common histopathological subtype reported in 35 (46.8%) biopsies. Other non-MCDs that followed were MGN in 11 (14.7%) children, MPGN and MSGN in 4 (5.3%) children each and IgA Nephropathy in one child (1.3%). One renal biopsy was consistent with congenital nephrotic syndrome (CNS) of Finnish type.
Discussion
Minimal change disease has been established as the most common cause of NS in children over the past three decades;[3] the incidence varies from 77 to 90% in different studies.[7810] However, changing trends in the histopathological patterns have been observed in the pediatric population over the past 30 years. Even in the earliest reports on renal biopsies in NS, FSGS was not uncommon. About 5–7% of renal biopsies performed for NS were consistent with this histopathological subtype.[71011] However, FSGS is becoming increasingly common in children with NS, warranting a renal biopsy on all such children for accurate diagnosis and management even in resource-limited settings like ours. A rising trend of FSGS and other non-MCD subtypes validates the need for renal biopsy in all children with NS. Our data are also consistent with the emergence of non-MCDs with FSGS as the most frequently reported histological subtype. In our study, renal biopsies on seventy-five children with NS were analyzed. There was a male predilection that is in accordance with the international data.[312] The mean age at onset was 11.2 ± 3.7 years. This is in contrast to the published data that reveal a younger age at onset of the disease.[231113] Most of the children in our study group were older than 10 years of age. A similar mean age has been described in a local study by Mubarak and Kazi.[14] Of the 75 cases of NS, 25 (33.3%) were steroid sensitive, 36 (48%) were steroid resistant, 10 (13.3%) were steroid dependent and 4 (5.3%) were with relapse. Data from Iran on children with NS reported different figures; 87% children were steroid sensitive, and 13% were found to be steroid resistant.[15] There is variation in the local data as well. Mubarak et al. also reviewed children with NS and reported 46.6% to be steroid dependent and 31% to be steroid resistant. The histopathology also varied according to the clinical subtype of NS. MCD was the most common subtype in steroid dependent NS; for all other clinical subtypes, FSGS was the leading pathological cause.[12] In our study, for all the clinical subtypes except relapse, FSGS was the most common histological lesion. MCD remained the most common underlying histological subtype for relapsed NS [Figure 1]. Studies from other countries have also reported FSGS as the leading cause of both idiopathic and difficult NS.[231617] However, data from different centers continue to report MCD as a common cause of NS in the pediatric group.[11181920] We also report a frequency of 1.3% of congenital NS that is almost similar to that reported in a local study by Mubarak et al.[12]
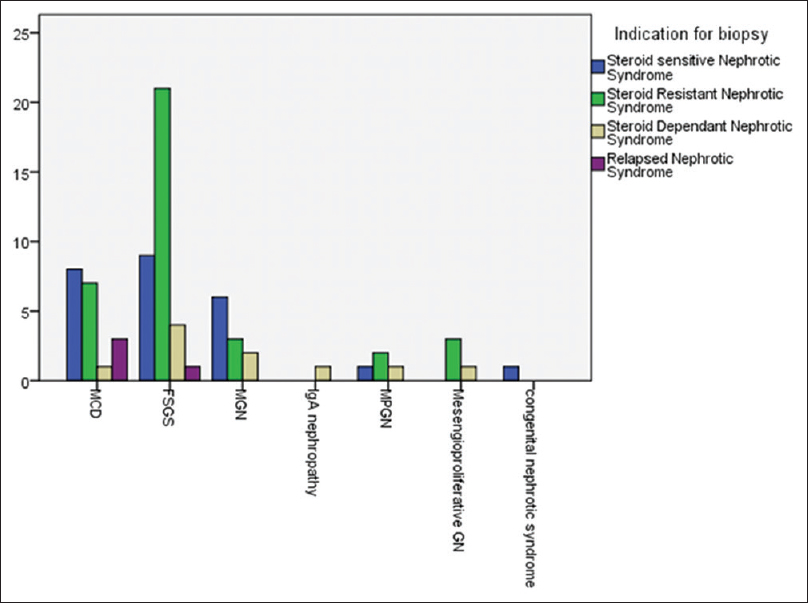
- Frequency of the different histopathological subtypes of nephrotic syndrome in relation to the clinical subtypes in children between 0-16 years of age. X-axis: histological subtypes, Y-axis: number of patients. Indications of renal biopsies related to color code on right side
Conclusion
In children, it is important to distinguish MCD from other causes of NS because the clinical course and management of both vary significantly. As the non-MCD subtypes are becoming increasingly common, a histological diagnosis is crucial to the management and outcome of the disease. With increasing trends of FSGS reported in our study, the need for a renal biopsy in children with NS could not be emphasized more. In resource-limited countries like ours, many children with NS are managed without a histological diagnosis. We, therefore, recommended renal biopsy on all children with NS in order to improve patient care and outcome.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Histopathological spectrum of childhood nephrotic syndrome in Indian children. Pediatr Nephrol. 2003;18:657-60.
- [Google Scholar]
- Changing patterns in the histopathology of idiopathic nephrotic syndrome in children. Kidney Int. 1999;55:1885-90.
- [Google Scholar]
- Renal biopsies in children. A twelve year review. Port J Nephrol Hypertens. 2010;24:215-21.
- [Google Scholar]
- Safety and complications of percutaneous kidney biopsies in 715 children and 8573 adults in Norway 1988-2010. Clin J Am Soc Nephrol. 2012;7:1591-7.
- [Google Scholar]
- Percutaneous renal biopsy of native kidneys: Efficiency, safety and risk factors associated with major complications. Arch Med Sci. 2011;7:823-31.
- [Google Scholar]
- Pathology of the nephrotic syndrome in children: A report for the International Study of Kidney Disease in Children. Lancet. 1970;760:1299-302.
- [Google Scholar]
- Nephrotic syndrome in children: Prediction of histopathology from clinical and laboratory characteristics at time of diagnosis. A report of the International Study of Kidney Disease in Children. Kidney Int. 1978;13:159-65.
- [Google Scholar]
- Revised guidelines for management of steroid-sensitive nephrotic syndrome. Indian J Nephrol. 2008;18:31-9.
- [Google Scholar]
- Clinicopathological study of nephrotic syndrome in childhood. Lancet. 1970;1:1353-9.
- [Google Scholar]
- High incidence of focal segmental glomerulosclerosis in nephrotic syndrome of childhood. Pediatr Nephrol. 1999;13:13-8.
- [Google Scholar]
- Histopathological spectrum of childhood nephrotic syndrome in Pakistan. Clin Exp Nephrol. 2009;13:589-93.
- [Google Scholar]
- Time trends and ethnic patterns of childhood nephrotic syndrome in Yorkshire, UK. Pediatr Nephrol. 2001;16:1040-4.
- [Google Scholar]
- Study of nephrotic syndrome in children: Importance of light, immunoflourescence and electron microscopic observations to a correct classification of glomerulopathies. Nefrologia. 2013;33:237-42.
- [Google Scholar]
- Do current recommendations for kidney biopsy in nephrotic syndrome need modifications? Pediatr Nephrol. 2002;17:404-8.
- [Google Scholar]
- Spectrum of biopsy-proven renal disease in the pediatric age group at King Hussein Medical Center. J Res Med Sci. 2007;14:34-7.
- [Google Scholar]
- Ten year experience of pediatric kidney biopsies from a single center in Pakistan. Indian J Nephrol. 2010;20:190-2.
- [Google Scholar]
- Experience of renal biopsy in children with nephrotic syndrome. Pediatr Nephrol. 2006;21:286-8.
- [Google Scholar]
- Fifteen years of kidney biopsies in children: A single center in Egypt. Saudi J Kidney Dis Transpl. 2014;25:1321-7.
- [Google Scholar]




