

Translate this page into:
Acute Kidney Injury by Near-drowning: From the Beach to the Hemodialysis Center: A Case Report
 , Kaoutar Errajraji1, Sara Anibar1, Marouane Jabrane1, Mohamed Arrayhani1
, Kaoutar Errajraji1, Sara Anibar1, Marouane Jabrane1, Mohamed Arrayhani1
Corresponding author: Mohammed Bouchoual, Department of Nephrology, SOUSS MASSA University Hospital, Faculty of Medicine and Pharmacy, Ibn-Zohr University, Agadir, Morocco. E-mail: m.bouchoual@uiz.ac.ma
-
Received: ,
Accepted: ,
How to cite this article: Bouchoual M, Ouazzani ME, Errajraji K, Anibar S, Jabrane M, Arrayhani M. Acute Kidney Injury by Near-drowning: From the Beach to the Hemodialysis Center: A Case Report. Indian J Nephrol. doi: 10.25259/IJN_433_2024
Abstract
Acute kidney injury (AKI) secondary to near-drowning is rarely described and poorly understood. Much of the literature on near-drowning has concentrated on the respiratory, cerebral, cardiac, and hematologic complications. Near-drowning-induced AKI is a heterogenous clinical entity. We report a case of near-drowning, which developed inisolated AKI due to acute tubular necrosis requiring dialysis.
Keywords
Acute kidney injury
Acute tubular necrosis
Hemodialysis
Near-drowning

Introduction
Acute kidney injury (AKI) secondary to near-drowning is rarely described and poorly understood. Only a few cases of severe isolated AKI resulting from near-drowning exist in the literature. Near-drowning-induced AKI is a heterogenous clinical entity. We report the case of a 36-year-old man admitted to the emergency department 96 h after a near-drowning incident for severe AKI.
Case Report
A 36-year-old patient with no notable pathological history was admitted to the emergency department with abdominal pain, nausea, and anuria. He was doing well until four days before admission when he went swimming in the lake with his friends. He was exhausted before he got back to the shore and was suffocating. He was briefly unconscious (about 3–4 min) until rescued by his friend.
On physical examination, he was conscious with a GLASCOW score of 15/15; anuric for more than 36 h before admission, blood pressure 127/59 mmHg, body temperature was normal, pulse 76 beats per minute, and peripheral oxygen saturation was 96%.
Biological tests performed in the emergency department revealed severe AKIN III renal failure, with serum creatinine level 11.48 mg/dL, severe metabolic acidosis, hemoglobin concentration of 13 g/dL, leukocyte count of 12,200/μL, no elevation of infectious or immunological marker, and a spot urine protein–creatinine ratio of 130 mg/g.
The remaining tests, including C-reactive protein (CRP), creatine phosphokinase (CPK), liver test, calcium and phosphorus levels, and kidney ultrasound were normal.
The initial management consisted of infusion of isotonic saline with hourly monitoring of diuresis and respiratory status. Twenty-four hours later, hourly urine output was less than 10 m despite bolus infusion of saline and continuous infusion of furosemide, with the presence of lung crackles. Chest X-ray initially showed mild pulmonary congestion with bilateral pleural effusion.
The patient needed six sessions of dialysis every 2 days. On the 10th hospital day, serum creatinine level was 4.15 mg/dL. Since there was no improvement for over a week, a renal biopsy was performed. The renal tubular epithelial cells were denuded and had exfoliating brush borders and intermittent mitosis due to regeneration. The interstitium was edematous and had mild infiltration of lymphocytes, but the glomeruli showed unremarkable finding [Figure 1], suggesting adiagnosis of acute tubular necrosis. The patient’s renal function recovered spontaneously, 1.54 mg/dL and 0.8 mg/dL 3 and 4 weeks later, respectively.
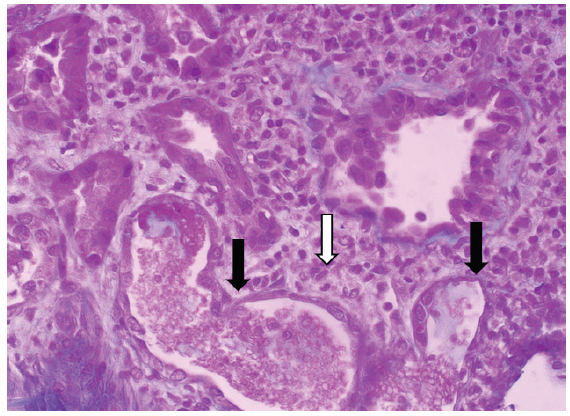
- Kidney biopsy specimen with PAS stain from the patient with serum creatinine of 2.48 mg/dL. Desquamation of epithelial cells within the tubular lumen, thinning of the tubular epithelium (black arrows) with the presence of a peritubular inflammatory infiltrate (white arrow) (× 400). PAS: Periodic acid-Schiff.
Discussion
Immersion or near-drowning can affect different major organ systems in the body. A retrospective study done by Spicer et al. at hospitals in Sydney found that AKI associated with near-drowning occurs in 50% of near-drowning emergency room admissions.1 Although the actual incidence of AKI following near-drowning is unknown, it is thought to be less frequent compared to lung, brain, or heart injury.2 Most AKI resulting from near-drowning are mild, reversible, and self-limited.1
The pathophysiology of near-drowning-related AKI is multifactorial.3 Pre-renal factors include hypovolemia, hypotension, and hypothermia. Near-drowning is associated with variable degrees of tissue hypoxia, and subsequent ischemic reperfusion injury is thought to be the predominant underlying pathophysiology. In some patients, AKI was secondary to rhabdomyolysis.4,5 Similar to our case, acute tubular injury was the most consistent finding among patients who underwent renal biopsy.1,6
It is also important to ascertain whether the patient was exposed to toxic substances like diesel oil during near-drowning. Li et al. reported a case of isolated AKI in a 43-year-old sailor after exposure to diesel oil in a shipwreck. Renal biopsy showed evidence of acute tubular injury, which could be partly attributed to hydrocarbon toxicity following skin and gastrointestinal absorption. The patient did not require dialysis and recovered completely within 2 weeks. It was similar to previous case reports of isolated AKI.6
Conclusion
Near-drowning-related AKI requiring hemodialysis is seldom reported in the literature. The diagnosis of acute renal failure should not be overlooked in patients with a history of immersion or near-drowning. Clinicians should be aware that these patients can present with AKI even after several days of immersion or near-drowning.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
References
- Acute renal impairment after immersion and near-drowning. J Am Soc Nephrol. 1999;10:382-6.
- [CrossRef] [PubMed] [Google Scholar]
- Near-drowning: Epidemiology, pathophysiology, and initial treatment. J Emerg Med. 1996;14:461-7.
- [CrossRef] [PubMed] [Google Scholar]
- Rhabdomyolysis associated with near-drowning. Am J Med Sci. 1999;318:201-2.
- [CrossRef] [PubMed] [Google Scholar]
- Acute renal failure secondary to rhabdomyolysis following near-drowning in sea water. J Assoc Physicians India. 2003;51:512-3.
- [PubMed] [Google Scholar]
- Acute renal failure after immersion in seawater polluted by diesel oil. Am J Kidney Dis. 1999;34:E26.
- [CrossRef] [PubMed] [Google Scholar]




