

Translate this page into:
An Updated Review of Membranous Nephropathy

Corresponding author: Orhan Efe, Divison of Nephrology, Department of Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts, United States. E-mail: oefe@mgh.harvard.edu
-
Received: ,
Accepted: ,
How to cite this article: Efe O, So PNH, Anandh U, Lerma EV, Wiegley N. An Updated Review of Membranous Nephropathy. Indian J Nephrol. 2024;34:105–18. doi: 10.25259/ijn_317_23
Abstract
Membranous nephropathy (MN) is one of the most common causes of nephrotic syndrome in adults. The discovery of phospholipase A2 receptor (PLA2R) as a target antigen has led to a paradigm shift in the understanding and management of MN. At present, serum PLA2R antibodies are used for diagnosis, prognostication, and guiding treatment. Now, with the discovery of more than 20 novel target antigens, antigen mapping is almost complete. The clinical association of certain antigens provides clues for clinicians, such as the association of nerve epidermal growth factor-like 1 with malignancies and indigenous medicines. Serum antibodies are detected for most target antigens, except exostosin 1 and 2 and transforming growth factor-beta receptor 3, but their clinical utility is yet to be defined. Genome-wide association studies and studies investigating environmental factors, such as air pollution, shed more light on the underpinnings of MN. The standard therapy of MN diversified from cyclical cyclophosphamide and steroids to include rituximab and calcineurin inhibitors over the past decades. Here, we provide a cutting-edge review of MN, focusing on genetics, immune system and environmental factors, novel target antigens and their clinical characteristics, and currently available and emerging novel therapies in MN.
Keywords
Membranous nephropathy
PLA2R antibodies
target antigens
genetic predisposition
environmental factors
immunosuppression
emerging therapies

Introduction
Membranous nephropathy (MN) is the second most common cause of nephrotic syndrome in adults after diabetic nephropathy.1,2 The pathological hallmark of MN includes subepithelial immunoglobulin (Ig) deposition, posing damage in glomerular basement membrane (GBM), foot process effacement, and high-grade proteinuria. Since first described by Dr. Bell in 1946 as a thickened GBM and vacuolization,3 the pathophysiology of MN has become more evident. The discovery of anti-phospholipase A2 receptor (PLA2R) antibodies in 2009 proved the concept of circulating antibodies targeting the endogenous podocyte antigens.4 Nowadays, PLA2R testing is widely available worldwide and used in diagnosis, prognostication, and therapeutic assessment. Subsequent studies elucidated many other target antigens, such as thrombospondin type 1 domain-containing 7A (THSD7A),5 nerve epidermal growth factor-like 1 (NELL1),6 and exostosin 1 (EXT1)/exostosin 2 (EXT2).7,8 The field continues to evolve as we learn more about the utilities of serum antibodies against diverse podocyte antigens and associated conditions. Recent studies shed light on the imbalance between the effector and regulatory arm of the immune system and the role of genetic risk factors and environmental factors in addition to conventional risk factors, including autoimmune diseases, infections, malignancy, and drugs. Concurrent with the discoveries of podocyte-targeting autoantibodies, B-cell depletion with rituximab and calcineurin inhibitors (CNIs) has become an essential part of the treatment. Here, we review the understanding of the underpinnings of MN, focusing on the role of the regulatory immune system, genetics, and environmental factors such as air pollution. We present the clinical and pathological features of novel target antigens. By reviewing the clinical trials, we examine currently available targeted immunosuppressive treatments, including anti-CD20 monoclonal antibodies and CNIs, and emerging therapies, such as those targeting plasma cells and complement systems.
Pathogenesis of MN
Decades ago, Heyman nephritis (induced by anti-megalin and anti-fraction 1A (Fx1A) antibodies) served as foundational models for understanding the key concepts in MN.9 The initial hypothesis of trapping circulating pre-formed immune complexes was refuted after delineating that megalin is expressed on rat podocytes and circulating antibodies attach megalin in situ.10 This concept was later proven in humans by identifying target podocyte antigens neutral endopeptidase11 and PLA2R.4 In MN, immune complexes are isolated into the subepithelial area, and the pathology usually lacks endo- or extra-capillary proliferation. Thus, the kidney injury is mainly driven by damage to the podocyte and GBM rather than inflammation.12 Many risk factors pose the break in immune tolerance and lead to the production of autoantibodies against podocyte antigens1 and complement pathway activation [Figure 1].13-17 In addition to enhanced effector T-cell responses,18-21 these predisposing factors include genetic polymorphisms in the immune system or podocyte proteins,22-26 overexpression of podocyte antigens, such as due to certain cancers which express NELL16,27 or potentially air pollution,28 and the deficiencies in regulatory T-(Tregs) and B-cells (Bregs).29-31
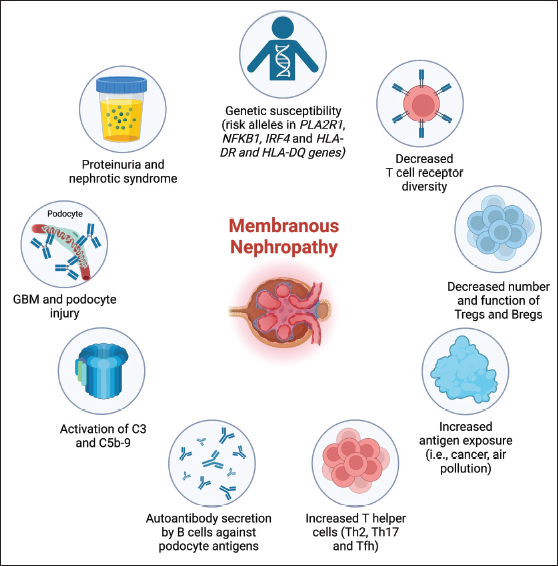
- Pathophysiological mechanisms of membranous nephropathy. Bregs: Regulatory B-cells, GBM: Glomerular basement membrane, Tfh: Follicular T helper cells, Th2: T helper 2, Th 17: T helper 17, Treg: Regulatory T-cells.
The Role of the Regulatory Immune System
Developing autoantibodies against the podocyte antigens is the key step in the pathogenesis of MN. How breaks occur in self-tolerance in MN remains speculative. The patients with MN had a lower Treg frequency and function and lower levels of inhibitory cytokine interleukin-35 than healthy controls, which improved after clinical remission post-immunosuppressive treatment.18,30 Rituximab responders had a significantly lower percentage of Tregs at baseline compared to non-responders.31 Mutation in key Treg genes such as FOXP3 can also induce an MN-like picture.32 Circulating Bregs were also lower in MN patients, and the number of Bregs negatively correlated with disease activity and improved post-treatment.29 Since Bregs also contribute to Treg differentiation, the inhibition of the two might be connected. In addition, to trigger an autoimmune response to an antigen, the amount of peptide is important. Increased expression of a certain peptide can activate effector T- and B-cells and overcome the suppression of the regulatory immune system. Representing this factor, increased air pollution reveals more PLA2R through an increased oxidative microenvironment,28 and cancer cells expressing NELL1 and THSD7A can induce MN. These factors, along with increased T helper 2,19 T helper 17,30 and follicular T helper cells,20 play a role in the failure of the regulatory immune system to suppress autoantibody production by B-cell lineage in MN.
The Role of Genetics and Environmental Toxins
MN is not inherited in a Mendelian fashion, but rather genetic risk variants predispose for disease development. Although some familial cases of MN were reported, they remain scarce and without a clear monogenic culprit.22,33,34
One aspect of high-risk genetic fingerprinting entails the genes of the immune system. Human leukocyte antigen (HLA) proteins present immunogens in their peptide grooves, and the type of HLA impacts the level of immune activation. Earlier studies showed an association of MN with HLA-DR3, HLA-DQA,24 and HLA-DQ1.25 Interestingly, the murine corresponding of HLA-DQ1 was associated with anti-GBM disease phenotype in mice.35 A recent genome-wide association studies (GWAS) discovered the risk HLA loci of DQA1*0501 in Europeans, DRB1*1501 in East Asians, and DRB1*0301 in both ancestries, explaining one-third of the disease risk.36 This study also discovered new risk alleles in NFKB1 and IRF4, encoding proinflammatory transcription factors. The same NKFB1 risk allele was found in ulcerative colitis and primary biliary cirrhosis, postulating its role in autoimmunity.37,38
Second, single-nucleotide polymorphisms of target antigens can predispose for MN, speculatively, by producing or revealing risk epitopes or antigen over-expression. The data from GWAS have shown a strong association of multiple PLA2R1 risk alleles on chromosome 2, through single-nucleotide polymorphism at intron and exon areas, and primary MN across different ethnic backgrounds.23,25,26 Supporting the role of PLA2R1 risk alleles, positive PLA2R antibody and increased glomerular PLA2R expression were found in ∼75% of the patients with risk variants while in none of the controls.26 Remarkably, the concordant presence of the HLA risk variants and the PLA2R1 risk allele was associated with an astronomical odds ratio for MN (78.5), indicative of strong genetic interaction.25 The risk variants related to other target antigens were not identified in GWAS. NELL1 was found to have a risk location in inflammatory bowel disease.39 In the future, genetic disease predictors will likely enhance the non-invasive diagnosis of MN.
The role of environmental factors in MN was studied scarcely. In China, the frequency of MN increased over a decade in many cities and correlated with air pollution.28 Increased exposure to fine particulate matter of <2.5 μm (PM2.5) after adjusting for confounders, such as age and location, was associated with 14% higher odds for MN. In a French study, MN patients were found to work more often in the construction sector and were frequently exposed to toxic substances, such as asbestos, lead, or organic solvents, compared to the general population.40 This was associated with epitope spreading in PLA2R-associated patients. More studies have yet to define the connection between pollution and MN.
Target Autoantigens
Within the past two decades, the discoveries of many target antigens advanced our understanding of MN dramatically [Figure 2]. First, Debiec et al. identified transplacental anti-neutral endopeptidase antibody-induced MN in a newborn with nephrotic syndrome whose mother had a genetic deficiency of neutral endopeptidase, proving target podocyte antigen theory in human.11 The paradigm shift occurred with the discovery of anti-PLA2R antibodies in 2009 by Beck et al., where they mixed serum of MN patients with normal glomerular extract and isolated PLA2R from immunoprecipitants with mass spectrometry.4 PLA2R-associated MN comprises ∼70% of MN cases and usually lacks a secondary cause. TSHD7A was discovered using a similar technique in 2014.5 Starting in 2019, Sethi et al. discovered many target antigens based on their higher expression in glomeruli of MN patients using mass spectrometry of micro-dissected glomeruli from biopsy materials,7 including EXT1/EXT2,8 NELL1,6 semaphorin-3B,41 protocadherin 7 (PCDH7),42 protocadherin FAT1 (FAT1),43 neuron-derived neurotrophic factor (NDNF) 3,44 and proprotein convertase subtilisin/kexin type 6 (PCSK6).45 In parallel, Al-Rabadi et al. and others have discovered other target antigens by immunoprecipitating immune complexes from frozen biopsy tissue and mass spectrometry of the immunoprecipitants. This method led to the discovery of serine protease HTRA1,46 contactin 1 (CNTN1),47 netrin G1 (NTNG1),48 transforming growth factor-beta receptor 3 (TGFBR3),49 and neural cell adhesion molecule 1 (NCAM1).50 Later, 17 more putative antigens were identified by Caza et al.51 and Sethi and Madden,52 which are yet to be confirmed. So far, the discovered target antigens comprise approximately 90% of cases of MN. Most of these antigens have concomitant circulating autoantibodies, and some are associated with specific etiologies, as summarized in [Figure 3]. Meanwhile, the field is moving toward the new classification system,53 and using working algorithms that rely on target antigens.52,54

- Timeline of identification of target antigens in membranous nephropathy. BSA: Bovine serum albumin, CD206: Cluster of differentiation 206, CNTN1: Contactin 1, EEA1: Early endosome antigen 1, EXT1/EXT2: Exostosin 1/2 complex, FAT1: Protocadherin FAT1, FCN3: Ficolin 3, HTRA1: Serine protease HTRA1, MST1: Macrophage stimulating 1, NCAM1: Neural cell adhesion molecule 1, NDNF: Neuron-derived neurotrophic factor, NELL-1: Neural epidermal growth factor-like 1, NPR3: Natriuretic peptide receptor 3, NTNG1: Netrin G1, PCDH7: Protocadherin 7, PCSK6: Proprotein convertase subtilisin/kexin type 6, PLA2R: Phospholipase A2 receptor, Sema3B: Semaphorin 3B, SEZ6L2: Seizure-related 6 homolog like 2, TGFBR3: Type III transforming growth factor-beta receptor, THSD7A: Thrombospondin type 1 domain-containing 7A, VASN: Vasorin.

- Etiological association of target antigens in membranous nephropathy. CDIP: Chronic inflammatory demyelinating polyneuropathy, HSCT: Hematopoietic stem cell transplant, BSA: bovine serum albumin; CNTN1: contactin 1; EXT1/EXT2: exostosin 1/2 complex; FAT1: protocadherin FAT1; NCAM1: neural cell adhesion molecule 1; NDNF: neuron-derived neurotrophic factor; NELL-1: neural epidermal growth factor-like 1; PCDH7: protocadherin 7; PCSK6: proprotein convertase subtilisin/kexin type 6; PLA2R: phospholipase A2 receptor; Sema3B: semaphorin 3B; TGFBR3: type III transforming growth factor-beta receptor; THSD7A: thrombospondin type 1 domain-containing 7A, NSAID: Non-steroidal anti-inflammatory drug.
NELL1 Association with Malignancy, Supplements, and Indigenous Medicines
NELL1 is the second most common target antigen in MN after PLA2R.6,27 NELL1-MN has shown association with malignancy, use of indigenous medicines, and use of lipoic acid.6,27,55,56 Original discovery cohort of NELL1-associated MN had no malignancy (0/29) but 4 of 5 patients had malignancy in the validation cohort.6 Caza et al. reported 33% (30/91) malignancy in NELL1 positive cases, mostly solid organ tumors, and a temporal correlation of MN with tumor incident.27 On the other hand, none of the NELL1-MN cases had malignancy in Chinese and Japanese cohorts, implicating race-based differences.57,58 As tumor tissues can express NELL1,27 the hypothesis for NELL1-associated MN in cancer patients includes a break in immune tolerance due to antigen overexpression and trapping of circulating antigens and/or immune complexes. Malignancy was also observed in MN with other target antigens, such as PCHD742 and THSD7A,5 but the significance of these associations yet to be determined.
NELL1 was also found in MN cases associated with mercury-containing indigenous medicines. The development of florid MN secondary to medicines prepared by practitioners of Siddha has gained attention in recent years. Siddha is a traditional medicine originating in South India and used for various indications such as sinusitis, skin lesions, bronchitis, and breast cancer. These recipes combine herbs and inorganic chemical compounds such as sulfur and mercury, which generate toxicities.59,60 Rasagandhi Mezhugu, another herbal-mineral combination, was associated with MN, again connected to the mercury content of the medicine. This remedy exposes 9–13.1 mg of mercury daily, which is much higher than the daily permissible limit of 0.003 mg.59 In a recent study of MN patients from India, one-third had a history of using traditional medicines that contain mercury such as Siddha and Ayurveda medicines.56 The majority of these cases were NELL1-positive (87.9%), while ∼10% were PLA2R-positive, and 3% were double-positive for NELL1 and PLA2R. The median duration of use was 5 months, and most patients underwent remission after discontinuation of the culprit medicines. Hypothesized mechanisms entail that mercury can interact with negatively charged GBM and alter GBM structure similar to the other cationic substances, such as gold, lipoic acid, and cationic bovine serum albumin, and activate the effector immune system.56,61
Lipoic acid is a popular over-the-counter antioxidant and insulin-mimetic supplement. It is under investigation in several conditions, including multiple sclerosis and diabetes.62 Case series of lipoic acid-induced MN showed an association with NELL1 (n = 7), with disease onset at 3–12 months after starting lipoic acid.55 Most cases showed an improvement in proteinuria after discontinuation. The underlying mechanism is unknown but likely similar to mercury-induced NELL1-MN. Other associations of NELL1-MN include non-steroidal anti-inflammatory drugs (NSAIDs)58 and tiopronin, a thiol agent used in the treatment of cystinuria.63
Target Antigens in Autoimmune Diseases
Exostosins are glycosyltransferases that are expressed in podocytes and responsible for the synthesis of the heparin sulfate backbone by adding glycosaminoglycan residues to core proteins. Presence of autoimmune diseases was prevalent in 81% of EXT1/EXT2-associated MN, including lupus and mixed connective tissue disorder, at a mean age of 36 years which is younger than primary MN.8 Remarkably, 35% of the lupus-associated MN was positive for EXT1/EXT2. The subepithelial location of EXT/EXT2 in biopsy series postulates the shedding of these proteins from podocytes. NCAM1 and TGFBR3 were also associated with membranous lupus nephritis, comprising ∼6% each.49,50 Intriguingly, considering neuronal expression of NCAM1, higher neuropsychiatric lupus was observed in NCAM1-MN, but this is still to be proven.50 CNTN1-positive MN was observed in patients with chronic inflammatory demyelinating polyneuropathy.47 In PCDH7-associated MN, ∼20% of patients had an autoimmune disease history.42 FAT1-MN was associated with hematopoietic stem cell transplant in a case series postulating its association with alloimmunity.43
Target Antigens in Infection- and Medication-Induced MN
Infections, including viral, bacterial, and parasites, can cause MN. Some viral infections including hepatitis B, hepatitis C, and human immunodeficiency viruses can be associated with PLA2R and THSD7A.64 In Schistosoma mansoni infection, MN cases exhibited features of primary MN, including PLA2R staining.65 The cases of syphilis-associated MN were associated with NDNF-3.44 In medication-induced MN, NSAID-associated cases showed a diverse antigen association. In a retrospective cohort, positive PLA2R staining was found in 50–75%.66 A novel target antigen, PCSK6, was also associated with prolonged NSAID intake in PLA2R-negative cases.45 Some cases were also associated with NELL1.58 A supplemental drug, lipoic acid, and mercury-containing indigenous medicine were reported in NELL1-associated MN as above.55 In childhood MN, cationic bovine serum albumin and corresponding antibodies were detected in serum and GBM, likely posed by cow milk intake in childhood MN.67
Kidney Pathology Considering Novel Target Antigens
The hallmark of MN is global and diffuses GBM thickening and subepithelial deposits containing immunoglobulin G (IgG). The IgG subtypes are usually IgG1 and IgG4, and there is scant C3 deposition postulating the involvement of the complement system in primary MN. Presence of concomitant immunoglobulin A (IgA), immunoglobulin M (IgM), and C1q deposition and IgG1, IgG2, and IgG3 subclasses reflect autoimmune diseases-associated MN, most commonly class V lupus nephritis.68 Electron microscopy can delineate the location and chronicity of deposits [Figure 4], aiding clinical decision-making.

- Pathologic stages of membranous nephropathy. Stage 1 involves a few small electron-dense deposits (EDDs) that are commonly inconspicuous under light microscopy. Stage 2 exhibits a greater deposition of EDDs accompanied by reactions from the surrounding GBM matrix, resulting in projections visualized as spikes on silver stain. Stage 3 includes the complete envelopment of the deposits, forming intramembranous EDDs and a laddering appearance. In stage 4, the rarefication of previously electron-dense deposits leads to an irregularly thickened GBM. An additional stage 0 was described in kidney allografts where fine IgG can be detected by immune fluorescence but not through electron microscopy, indicating a very early disease. EDD: Electron-dense deposit, GBM: Glomerular basement membrane, IgG: Immunoglobulin G.
Many of the target antigens were discovered by mass spectrometry due to their overexpression in MN.7 Taking advantage of the overexpression phenomenon, colocalizing IgG with PLA2R through immunofluorescence (IF) staining has become standard in the pathological evaluation of PLA2R-associated MN. In a similar approach, staining for a broader panel of target antigens is becoming standard when logistically available.52
THSD7A,5 NTNG1,48 and HTRA1-associated MN46 are all likely part of the primary MN in the conventional classification as they exhibit similar pathological features with PLA2R-MN, including diffuse granular IgG deposition comprising mainly IgG4 subclass that overlaps with linear antigen staining. Dual THSD7A and PLA2R staining is rare (1%).69 IgG4 subclass predominance is also observed in CNTN1,47 FAT1,43 cationic bovine albumin,67 and PSCK645 despite their secondary associations. In CNTN1, the association of mild disease with IgG4 was atypical compared to PLA2R-MN where the predominant Ig is IgG1 in mild and early disease, while IgG4 in later stages.47,70
Despite its secondary associations, NELL1-associated MN exhibits similar pathological characteristics to PLA2R-MN except for the segmental distribution of IgG.6,27 In EXT1/EXT2-associated MN, there is granular staining for EXT1 and EXT2 along the GBM without mesangial or extraglomerular staining along with all four IgG subclasses, the most abundant being IgG1 and IgG2.8,58 Given the autoimmune nature of EXT1/EXT2-associated cases, there is often concomitant staining of IgA, IgM, C3, and C1q across the glomerulus, including subepithelial, subendothelial, and mesangium, and tubuloreticular inclusions. NCAM150 and TGFBR3-associated MN49 exhibit features of membranous lupus nephritis. IHC staining of these two antigens is mostly global but can rarely be segmental and can include a tubular basement membrane. Predominant subepithelial IgG subclasses include IgG1, IgG2, and IgG3. EXT1/EXT2 and NCAM1 can also be associated with mixed proliferative and membranous lupus nephritis. In FAT1-associated MN, mostly in hematopoietic stem cell transplant recipients, pronase digestion was key for revealing FAT1 staining, given high glycosylation and the large molecule size.43 PCDH7-MN, which can be associated with non-lupus autoimmune diseases, showed heterogenous IgG subclass predominance and less prominent C3 staining.42 More progress in understanding the pathological features of rarer antigens will allow better categorization and disease patterns and, thus, personalized management.
Utility of Serum Antibodies for Target Antigens
Historically, the MN diagnosis has been made solely based on a kidney biopsy. This practice has changed since the discovery of anti-PLA2R antibodies. Given its high sensitivity and specificity, 60–70% and 90–100% for PLA2R-MN, respectively, the use of anti-PLA2R antibodies for diagnosis has become a gold standard.71 The studies have shown decreased test specificity in cases with decreased kidney function and other autoimmune diseases or diabetes.72 Thus, kidney disease: improving global outcomes (KDIGO) suggest obtaining a kidney biopsy despite a positive serum anti-PLA2R antibody when there is estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2, unusual clinical course, other serological abnormalities such as positive ANA, and unresponsiveness to immunotherapy therapy despite the disappearance of anti-PLA2R antibodies.73 PLA2R antibodies are also utilized for prognostication as high PLA2R antibody titers (>150 RU/mL) predict the extent of kidney injury.73 Finally, PLA2R antibodies predict response to treatment, as serological response precedes clinical response several months, and clinical relapse.74
Serum antibodies were also detected for many other target antigens in non-PLA2R-associated MN. Yet, none has been investigated for sensitivity or specificity due to their low prevalence. Although anti-THSD7A antibodies showed relatively good diagnostic association, the data are scarce.75,76 KDIGO considers available evidence insufficient for serology-based diagnosis in THSD7A-MN.73 Circulating antibodies against HTRA1 showed a negative correlation with disease activity.46 The utility of other positive circulating antibodies, such as anti-NELL1, PCDH7, FAT1, CNTN1, and NTNG1 antibodies, remains to be enlightened.6,42,43,47,48 So far, serum anti-exostosin8,58 and anti-TGFBR349 antibodies have not been detected, which could be a kidney sink effect or the unavailability of epitopes in vitro.
Immunosuppressive Treatment in the Current Era
The primary objectives of the MN treatment are to halt the advancement of kidney disease, mitigate the adverse effects of nephrotic syndrome, and enhance quality of life by reducing symptoms. These goals are achieved through a multifaceted approach, including supportive and, often, immunosuppressive therapy. This approach should consider the presence of secondary culprits such as malignancies, autoimmune diseases, infections, and culprit medications, especially in cases associated with pertaining target antigens.
Renin-angiotensin system (RAS) blockers, such as angiotensin-converting enzyme inhibitors and angiotensin receptor blockers, are the cornerstone of conservative management. In recent years, sodium-glucose cotransporter 2 inhibitors have emerged as a promising adjunctive therapy to RAS blockers in managing MN. In recent groundbreaking randomized clinical trials, dapagliflozin and empagliflozin improved proteinuria and decelerated eGFR decline in patients with proteinuric chronic kidney disease (CKD), including a total of 136 patients with MN.77,78 The associated nephrosis should be treated with diuretic therapies, lipid-lowering agents, and anticoagulation.
Immunosuppressive treatment is fundamental in patients who are at risk of progressive kidney function loss and severe complications of nephrotic syndrome. On the other hand, 30% of MN patients can have spontaneous remission within 6 months.79 It is prudent to consider the patient’s clinical characteristics when deciding on immunosuppression. At present, there are no standardized risk prediction tools.80,81 KDIGO categorizes patients into low, moderate, high, and very high risk based on clinical and biological markers [Figure 5].73 Immunosuppressive therapy is suggested in patients with moderate (optional), high, and very-high risk.
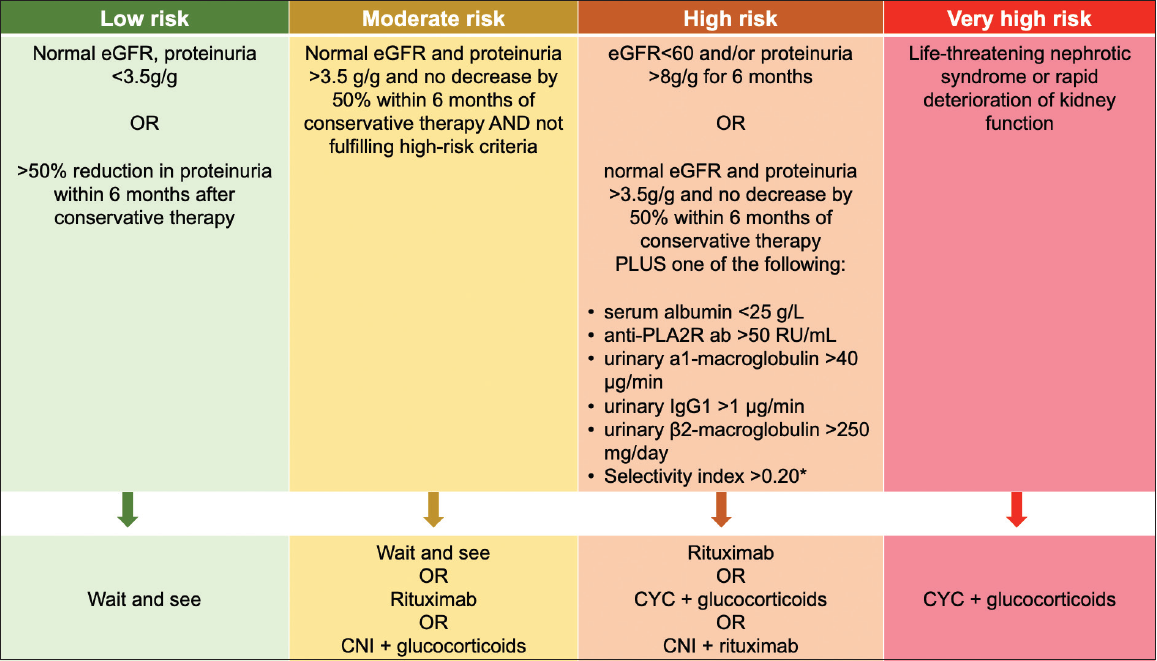
- Risk stratification and treatment options in membranous nephropathy. Modified from KDIGO 2021 Glomerular Disease Guideline.73 CNI: Calcineurin inhibitor, CYC: Cyclophosphamide, eGFR: Estimated glomerular filtration rate, PLA2R: phospholipase A2 receptor; IgG: immunoglobulin G. *Calculated by clearance of IgG/clearance of albumin.
The cyclical combination of alkylating agents, chlorambucil or cyclophosphamide, and steroids was the first effective immunosuppressive treatment in MN.82,83 The cyclical regimen is also associated with sustained remission in long term.84-86 However, the cyclical regimen is associated with toxicities such as infection, malignancy, and infertility. In parallel to the discovery of target antigens within the past two decades, the standard of care shifted toward more targeted therapies, including B-cell depletion with rituximab and CNIs based on landmark clinical trials [Table 1]. At present, cyclical cyclophosphamide + steroid is reserved for very high-risk patients.73 The choice of therapy is also affected by other factors, such as drug availability, patient preference, and reimbursement policies. Below, we present cutting-edge treatment options and emerging therapies for MN.
Rituximab
Rituximab is a chimeric, monoclonal anti-CD20 IgG1 antibody that depletes B-cells for 6–8 months post-infusion.87 Rituximab kills a broad spectrum of B-cells, from pro-B-cells to memory B-cells, which reduces serum PLA2R antibodies, but not plasmablasts or plasma cells.88 The role of anti-CD20 agents was further supported by the correlation of PLA2R antibodies and disease activity. Rituximab has long been investigated in antibody-mediated autoimmune diseases, including MN.88 In 2002, the first study investigating rituximab in eight MN patients showed its success in reducing proteinuria.89 This success was replicated in many uncontrolled and controlled trials, which made rituximab a first-line therapy in MN [Table 1].90,91 First, the GEMRITUX trial showed the efficacy of rituximab compared to supportive therapy, inducing ∼65% partial or complete remission at 17 months.92 MENTOR trial showed a superior sustained remission at 2 years in rituximab-treated patients compared to cyclosporin therapy (60% and 20%, respectively).87 The RI-CYCLO trial compared rituximab with the Ponticelli cyclical regimen.93 Although complete remission at 12 months was higher in the cyclic regimen arm (32% vs. 16%), the probabilities of complete or partial remission were similar at 2 years (82% vs. 83%). The serious adverse effects were similar in both groups. Overall, these outcomes implicate the efficacy of rituximab for both induction and maintenance of remission. Although there is a lack of long-term follow-up data, rituximab monotherapy was associated with a 5% relapse rate after remission compared to a 50% relapse in the cyclosporin group at 2 years.87
Since remission induction can be delayed in rituximab-treated patients, the short-term addition of bridging therapies was considered. Supporting this idea, a retrospective study by Zonozi et al. showed 100% remission rate with the combination of rituximab with low-dose cyclophosphamide for 2 months and (2.5 mg/kg oral daily for 1 week, then 1.5 mg/kg oral daily at weeks 2–8) and a rapid prednisone taper.94 On the other hand, addition of an upfront tacrolimus before rituximab infusion at 6 months was found inferior to the cyclical regimen for remission induction at 2 years in the STARMEN trial.95 Hypogammaglobulinemia and associated infection risk, especially during the COVID-19 pandemic, infusion reactions, and the requirement of an infusion center can limit the use of rituximab.
A total of 20–30% of MN patients have resistance to treatment. Although the incidence is unknown, some of this resistance originates due to rituximab resistance depicted by failure to deplete B-cells, rapid return of B-cells, and lack of efficacy.96 Chimeric structure and predominantly complement-mediated B-cell killing play a role in rituximab resistance by causing anti-rituximab antibody formation and ineffective B-cell killing, respectively.97 The required frequency and dose of rituximab in these cases are yet to be defined. In rituximab-resistant cases, fully humanized and more potent anti-CD20 agents such as obinituzumab and ofatumumab can be utilized, as discussed below.98-104
CNIs
CNIs have the advantage of inhibiting T-cells, blocking T- and B-cell interactions, and stabilizing the podocyte cytoskeleton by preserving synaptopodin. CNIs have shown efficacy in MN in remission induction [Table 1].105 However, the high relapse rate (up to 50%) after medication withdrawal, even when combined with steroids, makes CNIs less favorable compared to rituximab and, sometimes, cyclical regimens.106 High rate of relapse was observed with both short-term (i.e., 6-month cyclosporin) and long-term treatments. Praga et al. showed the efficacy of tacrolimus over supportive care in a randomized trial but at the expense of a high relapse rate [Table 1].107 The STARMEN trial compared low-dose tacrolimus (0.05 mg/kg/day for 6 months and tapering for another 3 months) plus 1 g of rituximab at month 6 with a modified Ponticelli regimen (corticosteroids alternating monthly with oral cyclophosphamide for 6 months).95 Complete or partial remission was achieved in 58% and 84% in tacrolimus-rituximab and cyclophosphamide-corticosteroid groups, respectively, at 2 years, implicating the superiority of cyclophosphamide-corticosteroid treatment [Table 1]. However, relapse rates were low and similar between the groups, which postulate the addition of rituximab can overcome the high risk of relapse. The efficacy of CNIs was also inferior in sustaining the remission in the long-term compared to the cyclic regimen with cyclophosphamide and steroids at 6 years post-treatment, 62% versus 28%, respectively.85 Effective CNI regimens can include both tacrolimus 0.05–1 mg/kg/d aiming of 3–8 ng/mL, or cyclosporin 3.5 mg/kg/d with a goal of 125–225 ng/mL for 12 months. It is often used with low-dose prednisone (i.e., 10 mg/day). The CNIs can be withdrawn if there is no response for 4 months and tapered to lower levels after 12 months in responsive patients. Kidney toxicity, hypertension, or the requirement of monitoring blood levels remain a barrier for use of CNIs in some patients.
Treatment in MN with Kidney Dysfunction
Reduced kidney function poses a higher risk end-stage kidney disease in MN [Figure 5]. Even if remission is achieved, these patients may remain with a lesser residual kidney function to tolerate another recurrence. Moreover, patients with eGFR <30 mL/min/1.73 m2 are rarely included in clinical trials. The risk and benefits of immunosuppression have been debated in patients with extensive chronicity in biopsy. Thus, reduced kidney function deserves special consideration in MN.
In a remote randomized trial in MN with progressive kidney disease, 20% decline in kidney function was observed in 58% of patients who were treated with cyclical steroid and chlorambucil, which was superior to both controls and cyclosporin-treated patients (84% and 81%, respectively).108 In a retrospective study, the use of extended cyclophosphamide (12 months) and steroids in patients with eGFR <70 mL/min (n = 59) was able to attain remission or stabilization of kidney function in all patients at the expense of high adverse events. However, it was associated with a relatively high rate of relapse with a cumulative incidence of 28% at 5 years.109 Rituximab treatment also achieved stabilization or improvement of eGFR in PLA2R-associated MN patients with eGFR <30 mL/min/1.72 m2.110 However, in patients with high chronicity in kidney biopsy, proteinuria improvement was less pronounced in patients treated with rituximab.111 The combination regimen of Zonozi et al. (rituximab, cyclophosphamide, and prednisone), induced 100% partial or complete remission, implicating the efficacy of this strategy. Forty-three percentages of the patients had a baseline eGFR of <60 mL/min/1.73 m2 in this study.94
In light of these data, KDIGO recommends rituximab or cyclophosphamide and steroid regimens in patients with high risk and reduced eGFR. Suppose serum PLA2R antibodies persist at 6 months. In that case, a second cycle of rituximab should be used in patients treated with rituximab, and rituximab can be added for patients who are treated with a cyclophosphamide-based regimen. In cases facing rituximab resistance and failure to achieve full B-cell depletion, more potent anti-CD20 agents such as obinutuzumab can be utilized, given their success in refractory MN.98,99,101-104 CNIs should be reserved only for intolerance to or unavailability of other agents, given their inferiority and higher risk of relapse. Future therapies might expand available options for MN patients with high risk.
Emerging Therapies
Alternative therapies are needed in MN given the failure to induce remission in 20–30% and the risk of relapse. Potential future therapies in MN will target B-cells and plasma cells to block antibody production and complement pathways. Moreover, resistance to rituximab and associated severe infusion reactions postulate the need for more potent alternative anti-CD20 agents.
Obinutuzumab and ofatumumab are fully humanized anti-CD20 antibodies, which are expected to have lower rates of severe infusion reactions and less treatment resistance.97 Obinutuzumab has an enhanced antibody-dependent cytotoxicity and induces a more potent B-cell depletion in blood and secondary lymphoid organs.112 Ofatumumab has a binding site for C1q and exhibits a stronger complement-mediated cytotoxicity.97 Reflecting their potential, both obinutuzumab98,99,101-103 and ofatumumab104 showed efficacy in refractory MN and nephrotic syndrome following a potent and prolonged B-cell depletion. At present, there are two ongoing trials with obinutuzumab in MN (NCT04629248, NCT05050214), the latter is investigating its efficacy in rituximab-resistant patients [Table 2].
Belimumab is a monoclonal antibody against B-lymphocyte stimulator (BLyS), a survival and development cytokine for B-cells. Belimumab has shown efficacy in lupus nephritis as an add-on therapy.113 In a single-arm pilot study, belimumab also showed efficacy in PLA2R-MN by reducing PLA2R antibody titers and achieving partial or complete remission.114 In light of these findings, an ongoing trial is investigating the effectiveness of belimumab combined with rituximab, compared with rituximab alone (NCT03949855) [Table 2]. Another trial is investigating the efficacy of povetacicept, a dual BLyS/APRIL inhibitor in PLA2R-MN (NCT05732402) [Table 2].
Considering the substantial and sustained antibody production by plasma cells, studies examining the efficacy of anti-plasma cell agents are sought in MN, like other antibody-driven glomerulonephritis. The cutting-edge anti-plasma cell agents target CD38 on plasma cells, including daratumumab, isatuximab, and felzartamab. Felzartamab is examined in MN in the phase 1b/2a and the phase 2 studies of PLA2R-MN and showed a dose-dependent reduction in serum anti-PLA2R antibodies (NCT04733040 and NCT04733040). Another study is investigating the effect of Felzartamab in MN (NCT04893096) [Table 2].
The role of complement system activation has been depicted both in pre-clinical and clinical studies.13-16 Although all three complement pathways are involved, the fingerprints of classical and lectin pathways were more pronounced in human samples.17 At present, there are two clinical trials examining the efficacy of complement inhibitors in MN, including iptacopan, a factor B inhibitor (NCT04154787), and narsoplimab, a monoclonal antibody inhibiting mannan-binding lectin serine protease 2, a serine protease responsible for cleavage of the complement components C2 and C4 (NCT02682407) [Table 2].
Further, therapeutic strategies are tested or hypothesized, which are still far from entering clinical practice. Immunoadsorption was tested in PLA2R-MN and reduced antibody titers quickly; however, it failed to improve surrogate endpoints.115 Other cutting-edge investigations include zanubrutinib, a Bruton’s tyrosine kinase inhibitor (NCT05707377); efgartigimod, an Fc receptor blocker (NCT05810961), and VB119, a monoclonal antibody which targets the CD19 epitope expressed on maturing B-cells including short-lived plasma cells (NCT04652570). CAR-T-cells to target PLA2R-peptide recognizing B-cells and sweeping antibody technology to clear circulating antigens are speculated but not tested in MN.116
| Regimen | Year | RCT | Control Arm | Treatment arm | Follow up | Remission | Relapse |
|---|---|---|---|---|---|---|---|
| Cytotoxic regimen | 1984 | Ponticelli et al.82 | Supportive therapy | Cyclical methylprednisolone (1 g x3) followed by prednisone (0.4 mg/kg/d) at months 1, 3, and 5 and chlorambucil (0.2 mg/kg/d) at months 2, 4, and 6 | 31 months (12 to 84 months) | 30% vs 72% (CR+PR) 7% vs. 38% (CR) | NA vs. 17% (31 months) |
| 1998 | Ponticelli et al.117 | Cyclical methylprednisolone (1 g x3) followed by prednisone (0.4 mg/kg/d) at months 1, 3, and 5 and chlorambucil (0.2 mg/kg/d) at months 2, 4, and 6 | Cyclical methylprednisolone (1 g x3) followed by prednisone (0.4 mg/kg/d) at months 1, 3, and 5 and cyclophosphamide (2.5 mg/kg/d) at months 2, 4, and 6 | >12 months | 82% vs. 93% (CR+PR) 27% vs. 37% (CR) | 30.5% vs 25% (6-30 months) | |
| CNIs | 2001 | Cattran et al.106 | Low dose prednisone (0.15 mg/kg/day up to a maximum dose of 15 mg for 6 months) | Cyclosporin (3.5 mg/kg/day for 26 weeks) + prednisone (0.15 mg/kg/day up to a maximum dose of 15 mg for 6 months) | 78 weeks (20 months) | 13% vs. 39% (CR+PR) 4% vs. 7% (CR) | 60% vs. 48% (78 weeks) |
| 2007 | Praga et al.107 | Supportive therapy | Tacrolimus (0.05 mg/kg/day) for 12 months followed by taper | 18 months | 30% vs. 76% (CR+PR) 13% vs. 32% (CR) | NA vs 47% (30 months) | |
| 2017 | GEMRITUX92 | Supportive therapy | Rituximab (375 mg/m2 x 2) | 17 months | 34.2% vs. 64.9% (CR+PR) 0% vs. 19% (CR) | N/A | |
| 2019 | MENTOR87 | Cyclosporin (3.5 mg/kg/d for 6 months with an additional 6 months if proteinuria is down by >25% but no complete remission) | Rituximab (1 gr x 2, with a second course at 6 months if proteinuria down by >25% but no complete remission) | 24 months | 20% vs. 60% (CR+PR) 0% vs. 35% (CR) | 53% vs 5% (24 months) | |
| Rituximab | 2020 | STARMEN95 | Cyclical methylprednisolone (1 g x3 followed by oral 0.5 mg/kg/d) at months 1, 3, and 5 and cyclophosphamide (1-2 mg/kg/d) at months 2, 4, and 6 | Tacrolimus (0.05 mg/kg/day) for 6 months followed by taper + Rituximab 1 g at 6 month | 24 months | 84% vs. 58% (CR+PR) 60% vs. 26% (CR) | 2.7% vs. 12% (24 months) |
| 2021 | RI-CYCLO93 | Cyclical methylprednisolone (1 g x3 followed by oral 0.5 mg/kg/d) at months 1, 3, and 5 and cyclophosphamide (2 mg/kg/d) at months 2, 4, and 6 | Rituximab (1 gr x2) | 36 months | 73% vs 85% (CR+PR) 32% vs. 30% (CR) | 22% vs 13% (36 months) |
NA: not applicable, CNI: Calcineurin inhibitor, CR: Complete remission, PR: Partial remission, RCT: Randomized controlled trial.
| Clinical Trial | Disease and Phase | Treatment arm | Control arm | eGFR cut off | Proteinuria cut off | Prior treatment | Primary outcome |
|---|---|---|---|---|---|---|---|
| NCT05050214 | MN, phase II | Obinutuzumab at days 0 (100 mg), 1 (900 mg), and weeks 2 and 4 (1000 mg each) | Single arm | >30 ml/min/1.73 m2 | >3.5 g/24 h | Rituximab resistance or failure | Partial or complete remission at 52 weeks |
| NCT04629248 | MN, phase III | Obinutuzumab at week 0, 2, 24, and 26 (1000 mg each) | Tacrolimus for 52 weeks | >40 ml/min/1.73 m2 | UPCR >5 g/g or >4 g/g depending on duration of supportive care | Supportive care for 3 or 6 months | Complete remission at 104 weeks |
| NCT03949855 | PLA2R-MN, phase II | Belimumab (subcutaneous 200-400 mg weekly for 52 weeks) + Rituximab (1000 mg at weeks 4 and 6 and potentially at 34 and 36) | Placebo+ Rituximab | >30 ml/min/1.73 m2 | 4-8 g/24 h or >8 g/24 h depending on duration of supportive care | Supportive care for 3 or 6 months | Complete remission at 104 weeks |
| NCT05732402 | MN, phase I and II | Povetacicept (subcutaneous 80 or 240 mg every 4 weeks for 6 to 12 months) | 2-arm | >30 ml/min/1.73 m2 | UPCR >1 g/g for PLA2R and THSD7A positive cases and UPCR >3.5 g/g for PLA2R and THSD7A negative cases | Supportive care for 3 months | Adverse events |
| NCT04145440 | PLA2R-MN, phase I and II | Felzartamab (4 doses weekly and 5 doses every 4 weeks) | Single arm | >50 ml/min/1.73 m2 and 30-50 if IFTA<25% | UPCR of >3.0 g/g or proteinuria >3.5 g/24 h | Supportive care per guidelines | Safety and tolerability |
| NCT04733040 | PLA2R-MN, phase II | Felzartamab (5 doses at days 1, 8, 15, 29, and 57 or 2 doses at days 1 and 15) | 2-arm | >50 ml/min/1.73 m2 and 30-50 if IFTA<25% | UPCR of > 3.0 g/g or proteinuria > 3.5 g/24 h | Supportive care per guidelines | percent change of anti- PLA2R antibody at 3 months |
| NCT04893096 | MN, Phase II | Felzartamab (weekly infusion for 4 weeks and then every 4 weeks for 5 doses) | 2-arm | >30 ml/min/1.73 m2 | >3.5 g/day and less than 50% reduction during rituximab treatment | Rituximab resistance or dependence | Partial or complete remission and change in proteinuria till 24 months |
| NCT02682407 | MN, Phase II | Narsoplimab for 12 weeks (subcutaneous or intravenous, dose unclear) | Single arm | >30 ml/min/1.73 m2 | >1 g/24 h | Supportive care (unclear duration) | Safety and tolerability |
| NCT04154787 | PLA2R-MN, phase II | Iptacopan oral for 24 weeks (dose unclear) | Rituximab | >30 mL/min per 1.73 m2 | >3.5 g/24 h | Supportive care for 8 weeks | Ratio between baseline and 24-week UPCR |
MN: membranous nephropathy; PLA2R-MN: phospholipase A2 receptor associated membranous nephropathy; UPCR: urine protein to creatinine ratio; THSD7A: thrombospondin type 1 domain-containing 7A; eGFR: estimated glomerular filtration rate.
Conclusion
As the underlying mechanisms become more evident with the discovery of novel target antigens, more diverse serum autoantibodies will potentially serve as biomarkers for diagnosis, treatment response, and relapse in MN, in addition to PLA2R. The field progressed swiftly, delineating the association of target antigens with corresponding culprits such as specific drug and malignancy associations, such as NELL1 in cancer and EXT1/EXT2 in autoimmune diseases. The state-of-the-art immunosuppressive treatment entails anti-CD20 monoclonal antibodies and CNIs while reserving conventional alkylating agents with steroids for high-risk patients. Future studies will diversify treatment options by adding more targeted strategies, including complement inhibitors and plasma cell targeting therapies.
Acknowledgments
Figures are created with Biorender.com.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- The czech registry of renal biopsies. Occurrence of renal diseases in the years 1994-2000. Nephrol Dial Transplant. 2004;19:3040-9.
- [CrossRef] [PubMed] [Google Scholar]
- Welcome collection. Available from: https://wellcomecollection.org/works/ga554zdb [Last accessed on 2023 Apr 02]
- [Google Scholar]
- M-type phospholipase A2 receptor as target antigen in idiopathic membranous nephropathy. N Engl J Med. 2009;361:11-21.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Thrombospondin type-1 domain-containing 7A in idiopathic membranous nephropathy. N Engl J Med. 2014;371:2277-87.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Neural epidermal growth factor-like 1 protein (NELL-1) associated membranous nephropathy. Kidney Int. 2020;97:163-74.
- [CrossRef] [PubMed] [Google Scholar]
- New “Antigens” in membranous nephropathy. J Am Soc Nephrol. 2021;32:268-78.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Exostosin 1/exostosin 2-associated membranous nephropathy. J Am Soc Nephrol. 2019;30:1123-36.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Heymann nephritis: Mechanisms of renal injury. Kidney Int. 1989;35:976-84.
- [CrossRef] [PubMed] [Google Scholar]
- Autologous immune complex nephritis induced with renal tubular antigen. I. Identification and isolation of the pathogenetic antigen. J Exp Med. 1968;127:555-72.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Antenatal membranous glomerulonephritis due to anti-neutral endopeptidase antibodies. N Engl J Med. 2002;346:2053-60.
- [CrossRef] [PubMed] [Google Scholar]
- Cellular response to injury in membranous nephropathy. J Am Soc Nephrol. 2005;16:1195-204.
- [CrossRef] [PubMed] [Google Scholar]
- Glomerular C3c localization indicates ongoing immune deposit formation and complement activation in experimental glomerulonephritis. Am J Pathol. 1993;142:179-87.
- [PubMed] [PubMed Central] [Google Scholar]
- IgG subclasses and complement pathway in segmental and global membranous nephropathy. Pediatr Nephrol Berl Ger. 2010;25:1091-9.
- [CrossRef] [PubMed] [Google Scholar]
- The membrane attack complex in complement-mediated glomerular epithelial cell injury: Formation and stability of C5b-9 and C5b-7 in rat membranous nephropathy. J Immunol. 1986;137:1511-6.
- [PubMed] [Google Scholar]
- A new role for complement in experimental membranous nephropathy in rats. J Clin Invest. 1980;66:1339-50.
- [CrossRef] [PubMed] [Google Scholar]
- The classical pathway triggers pathogenic complement activation in membranous nephropathy. Nat Commun. 2023;14:473.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- A comprehensive phenotypic and functional immune analysis unravels circulating anti-phospholipase A2 receptor antibody secreting cells in membranous nephropathy patients. Kidney Int Rep. 2020;5:1764-76.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Up-regulated interleukin-4 production by peripheral T-helper cells in idiopathic membranous nephropathy. Nephrol Dial Transplant. 2004;19:580-6.
- [CrossRef] [PubMed] [Google Scholar]
- Higher frequencies of circulating ICOS(+), IL-21(+) T follicular helper cells and plasma cells in patients with new-onset membranous nephropathy. Autoimmunity. 2017;50:458-67.
- [CrossRef] [PubMed] [Google Scholar]
- Helper T cells in idiopathic membranous nephropathy. Front Immunol. 2021;12:665629.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Genetics of membranous nephropathy. Nephrol Dial Transplant. 2018;33:1493-502.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- The genetic architecture of membranous nephropathy and its potential to improve non-invasive diagnosis. Nat Commun. 2020;11:1600.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- HLA Associations in end-stage renal disease due to membranous glomerulonephritis: HLA-DR3 associations with progressive renal injury. southeastern organ procurement foundation. Am J Kidney Dis. 1994;23:797-802.
- [CrossRef] [PubMed] [Google Scholar]
- Risk HLA-DQA1 and PLA(2)R1 alleles in idiopathic membranous nephropathy. N Engl J Med. 2011;364:616-26.
- [CrossRef] [PubMed] [Google Scholar]
- Interaction between PLA2R1 and HLA-DQA1 variants associates with anti-PLA2R antibodies and membranous nephropathy. J Am Soc Nephrol. 2013;24:1323-9.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- NELL1 is a target antigen in malignancy-associated membranous nephropathy. Kidney Int. 2021;99:967-76.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Long-term exposure to air pollution and increased risk of membranous nephropathy in china. J Am Soc Nephrol. 2016;27:3739-46.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Regulatory B cells are reduced and correlate with disease activity in primary membranous nephropathy. Kidney Int Rep. 2020;5:872-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Altered Th17/Treg ratio as a possible mechanism in pathogenesis of idiopathic membranous nephropathy. Cytokine. 2021;141:155452.
- [CrossRef] [PubMed] [Google Scholar]
- B- and T-cell subpopulations in patients with severe idiopathic membranous nephropathy may predict an early response to rituximab. Kidney Int. 2017;92:227-37.
- [CrossRef] [PubMed] [Google Scholar]
- Pathophysiological lessons from rare associations of immunological disorders. Pediatr Nephrol. 2009;24:3-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Familial membranous nephropathy: An X-linked genetic susceptibility? Nephron Clin Pract. 2008;108:C10-5.
- [CrossRef] [PubMed] [Google Scholar]
- Two brothers with idiopathic membranous nephropathy and familial sensorineural deafness. Am J Kidney Dis. 1990;15:269-72.
- [CrossRef] [PubMed] [Google Scholar]
- Susceptibility to anti-glomerular basement membrane disease and goodpasture syndrome is linked to MHC class II genes and the emergence of T cell-mediated immunity in mice. J Clin Invest. 1997;100:2263-75.
- [CrossRef] [PubMed] [Google Scholar]
- Gene panel analysis in a large cohort of patients with autosomal dominant polycystic kidney disease allows the identification of 80 potentially causative novel variants and the characterization of a complex genetic architecture in a subset of families. Front Genet. 2020;11:464.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- International genome-wide meta-analysis identifies new primary biliary cirrhosis risk loci and targetable pathogenic pathways. Nat Commun. 2015;6:8019.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Genome-wide association study identifies 12 new susceptibility loci for primary biliary cirrhosis. Nat Genet. 2011;43:329-32.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Systematic association mapping identifies NELL1 as a novel IBD disease gene. PLoS One. 2007;2:e691.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Toxic occupational exposures and membranous nephropathy. Clin J Am Soc Nephrol. 2022;17:1609-19.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Semaphorin 3B-associated membranous nephropathy is a distinct type of disease predominantly present in pediatric patients. Kidney Int. 2020;98:1253-64.
- [CrossRef] [PubMed] [Google Scholar]
- Protocadherin 7-associated membranous nephropathy. J Am Soc Nephrol. 2021;32:1249-61.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Hematopoietic stem cell transplant-membranous nephropathy is associated with protocadherin FAT1. J Am Soc Nephrol. 2022;33:1033-44.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Membranous nephropathy in syphilis is associated with neuron-derived neurotrophic factor. J Am Soc Nephrol. 2023;34:374-84.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Proprotein convertase subtilisin/kexin type 6 (PCSK6) is a likely antigenic target in membranous nephropathy and nonsteroidal anti-inflammatory drug use. Kidney Int. 2023;104:343-52.
- [CrossRef] [PubMed] [Google Scholar]
- Serine protease HTRA1 as a novel target antigen in primary membranous nephropathy. J Am Soc Nephrol. 2021;32:1666-81.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Contactin-1 is a novel target antigen in membranous nephropathy associated with chronic inflammatory demyelinating polyneuropathy. Kidney Int. 2021;100:1240-9.
- [CrossRef] [PubMed] [Google Scholar]
- Netrin G1 is a novel target antigen in primary membranous nephropathy. J Am Soc Nephrol. 2022;33:1823-31.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Transforming growth factor beta receptor 3 (tgfbr3)-associated membranous nephropathy. Kidney 360. 2021;2:1275-86.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Neural cell adhesion molecule 1 is a novel autoantigen in membranous lupus nephritis. Kidney Int. 2021;100:171-81.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Discovery of seven novel putative antigens in membranous nephropathy and membranous lupus nephritis identified by mass spectrometry. Kidney Int. 2023;103:593-606.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Mapping antigens of membranous nephropathy: Almost there. Kidney Int. 2023;103:469-72.
- [CrossRef] [PubMed] [Google Scholar]
- Membranous nephropathy: Classification redux? Mayo Clin Proc. 2021;96:523-5.
- [CrossRef] [PubMed] [Google Scholar]
- A target antigen-based approach to the classification of membranous nephropathy. Mayo Clin Proc. 2021;96:577-91.
- [CrossRef] [PubMed] [Google Scholar]
- Lipoic acid supplementation associated with neural epidermal growth factor-like 1 (NELL1)-associated membranous nephropathy. Kidney Int. 2021;100:1208-13.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Traditional indigenous medicines are an etiologic consideration for NELL1-positive membranous nephropathy. Kidney Int. 2022;102:1424-6.
- [CrossRef] [PubMed] [Google Scholar]
- Neural epidermal growth factor-like 1 protein-positive membranous nephropathy in chinese patients. Clin J Am Soc Nephrol. 2021;16:727-35.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Prevalence of neural epidermal growth factor-like 1- and exostosin 1/exostosin 2-associated membranous nephropathy: A single-center retrospective study in Japan. Sci Rep. 2022;12:2967.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Membranous nephropathy associated with indigenous indian medications containing heavy metals. Kidney Int Rep. 2020;5:1510-4.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Toxic nephropathy secondary to chronic mercury poisoning: Clinical characteristics and outcomes. Kidney Int Rep. 2022;7:1189-97.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- What can mercury teach us about membranous nephropathy and minimal change disease? Kidney Int Rep. 2022;7:1157-60.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Safety evaluation of α-lipoic acid supplementation: A systematic review and meta-analysis of randomized placebo-controlled clinical studies. Antioxidants (Basel). 2020;9:1011.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Segmental NELL-1 membranous nephropathy complicating tiopronin therapy. Kidney Int Rep. 2023;8:1683-6.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Membranous nephropathy associated with viral infection. Clin Kidney J. 2021;14:876-83.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- The immunohistological profile of membranous nephropathy associated with chronic schistosoma mansoni infection reveals a glomerulopathy with primary features. Kidney Int. 2019;96:793-4.
- [CrossRef] [PubMed] [Google Scholar]
- Membranous nephropathy and nonsteroidal anti-inflammatory agents. Am J Kidney Dis. 2013;62:1012-7.
- [CrossRef] [PubMed] [Google Scholar]
- Early-childhood membranous nephropathy due to cationic bovine serum albumin. N Engl J Med. 2011;364:2101-10.
- [CrossRef] [PubMed] [Google Scholar]
- Glomerular IgG subclasses in idiopathic and malignancy-associated membranous nephropathy. Clin Kidney J. 2015;8:433-9.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- THSD7A staining of membranous glomerulopathy in clinical practice reveals cases with dual autoantibody positivity. Mod Pathol. 2016;29:421-6.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- IgG subclass staining in renal biopsies with membranous glomerulonephritis indicates subclass switch during disease progression. Mod Pathol. 2013;26:799-805.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnostic accuracy of PLA2R autoantibodies and glomerular staining for the differentiation of idiopathic and secondary membranous nephropathy: An Updated Meta-analysis. Sci Rep. 2015;5:8803.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Noninvasive diagnosis of PLA2R-associated membranous nephropathy: A validation study. Clin J Am Soc Nephrol. 2021;16:1833-9.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- KDIGO 2021 clinical practice guideline for the management of glomerular diseases. Kidney Int. 2021;100:S1-276.
- [CrossRef] [PubMed] [Google Scholar]
- Anti-phospholipase A2 receptor antibody titer predicts post-rituximab outcome of membranous nephropathy. J Am Soc Nephrol. 2015;26:2545-58.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- An indirect immunofluorescence method facilitates detection of thrombospondin type 1 domain-containing 7A-specific antibodies in membranous nephropathy. J Am Soc Nephrol. 2017;28:520-31.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Tissue staining for THSD7A in glomeruli correlates with serum antibodies in primary membranous nephropathy: A clinicopathological study. Mod Pathol. 2018;31:616-22.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383:1436-46.
- [CrossRef] [PubMed] [Google Scholar]
- Empagliflozin in patients with chronic kidney disease. N Engl J Med. 2023;388:117-27.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Spontaneous remission of nephrotic syndrome in idiopathic membranous nephropathy. J Am Soc Nephrol. 2010;21:697-704.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Validation of a predictive model of idiopathic membranous nephropathy: Its clinical and research implications. Kidney Int. 1997;51:901-7.
- [CrossRef] [PubMed] [Google Scholar]
- Prognostic value of risk score and urinary markers in idiopathic membranous nephropathy. Clin J Am Soc Nephrol. 2012;7:1242-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Controlled trial of methylprednisolone and chlorambucil in idiopathic membranous nephropathy. N Engl J Med. 1984;310:946-50.
- [CrossRef] [PubMed] [Google Scholar]
- Membranous nephropathy: Response to steroids and immunosuppression. Am J Nephrol. 2008;1:11-6.
- [CrossRef] [PubMed] [Google Scholar]
- A randomized, controlled trial of steroids and cyclophosphamide in adults with nephrotic syndrome caused by idiopathic membranous nephropathy. J Am Soc Nephrol. 2007;18:1899-904.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term follow-up of cyclical cyclophosphamide and steroids versus tacrolimus and steroids in primary membranous nephropathy. Kidney Int Rep. 2021;6:2653-60.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- A 10-year follow-up of a randomized study with methylprednisolone and chlorambucil in membranous nephropathy. Kidney Int. 1995;48:1600-4.
- [CrossRef] [PubMed] [Google Scholar]
- Rituximab or cyclosporine in the treatment of membranous nephropathy. N Engl J Med. 2019;381:36-46.
- [CrossRef] [PubMed] [Google Scholar]
- B-cell-directed therapies for autoimmune disease. Nat Rev Rheumatol. 2009;5:433-41.
- [CrossRef] [PubMed] [Google Scholar]
- Rituximab for idiopathic membranous nephropathy. Lancet. 2002;360:923-4.
- [CrossRef] [PubMed] [Google Scholar]
- Rituximab in membranous nephropathy. Kidney Int Rep. 2021;6:881-93.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Rituximab therapy for membranous nephropathy: A systematic review. Clin J Am Soc Nephrol. 2009;4:734-44.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Rituximab for severe membranous nephropathy: A 6-month trial with extended follow-up. J Am Soc Nephrol. 2017;28:348-58.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Rituximab or cyclophosphamide in the treatment of membranous nephropathy: The RI-CYCLO randomized trial. J Am Soc Nephrol. 2021;32:972-82.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Combination of rituximab, low-dose cyclophosphamide, and prednisone for primary membranous nephropathy: A case series with extended follow up. Am J Kidney Dis. 2021;78:793-803.
- [CrossRef] [PubMed] [Google Scholar]
- The STARMEN trial indicates that alternating treatment with corticosteroids and cyclophosphamide is superior to sequential treatment with tacrolimus and rituximab in primary membranous nephropathy. Kidney Int. 2021;99:986-98.
- [CrossRef] [PubMed] [Google Scholar]
- Postulated mechanisms of resistance of B-cell non-hodgkin lymphoma to rituximab treatment regimens: Strategies to overcome resistance. Semin Oncol. 2014;41:667-77.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Anti-CD20 therapies in multiple sclerosis: From pathology to the clinic. Front Immunol. 2023;14:1004795.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- A child with semaphorin 3b-associated membranous nephropathy effectively treated with obinutuzumab after rituximab resistance. Pediatr Nephrol. 2024;39:305-8.
- [CrossRef] [PubMed] [Google Scholar]
- Obinutuzumab in frequently relapsing and steroid-dependent nephrotic syndrome in children. Clin J Am Soc Nephrol. 2023;18:1555-62.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Obinutuzumab rescue in rituximab resistant mixed cryoglobulinemia. Kidney Int Rep. 2021;6:865-6.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Obinutuzumab in refractory phospholipase A2 receptor-associated membranous nephropathy with severe CKD. Kidney Int Rep. 2023;8:942-3.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Treatment Resistant M-type phospholipase A2 receptor associated membranous nephropathy responds to obinutuzumab: A report of two cases. BMC Nephrol. 2022;23:134.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Obinutuzumab is effective for the treatment of refractory membranous nephropathy. Kidney Int Rep. 2020;5:1515-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Ofatumumab in rituximab-resistant and rituximab-intolerant patients with primary membranous nephropathy: A case series. Am J Kidney Dis. 2023;???:S0272-7.
- [CrossRef] [PubMed] [Google Scholar]
- A controlled trial of cyclosporine in patients with progressive membranous nephropathy. Canadian glomerulonephritis study group. Kidney Int. 1995;47:1130-5.
- [CrossRef] [PubMed] [Google Scholar]
- Cyclosporine in patients with steroid-resistant membranous nephropathy: A randomized trial. Kidney Int. 2001;59:1484-90.
- [CrossRef] [PubMed] [Google Scholar]
- Tacrolimus monotherapy in membranous nephropathy: A randomized controlled trial. Kidney Int. 2007;71:924-30.
- [CrossRef] [PubMed] [Google Scholar]
- Immunosuppression for progressive membranous nephropathy: A UK randomised controlled trial. Lancet. 2013;381:744-51.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Cytotoxic therapy for membranous nephropathy and renal insufficiency: Improved renal survival but high relapse rate. Nephrol Dial Transplant. 2004;19:1142-8.
- [CrossRef] [PubMed] [Google Scholar]
- Rituximab in patients with phospholipase A2 receptor-associated membranous nephropathy and severe CKD. Kidney Int Rep. 2020;5:331-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Rituximab for idiopathic membranous nephropathy: Who can benefit? Clin J Am Soc Nephrol. 2006;1:738-48.
- [CrossRef] [PubMed] [Google Scholar]
- A tale of two antibodies: Obinutuzumab versus rituximab. Br J Haematol. 2018;182:29-45.
- [CrossRef] [PubMed] [Google Scholar]
- Two-year, randomized, controlled trial of belimumab in lupus nephritis. N Engl J Med. 2020;383:1117-28.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of belimumab on proteinuria and anti-phospholipase A2 receptor autoantibody in primary membranous nephropathy. Nephrol Dial Transplant. 2020;35:599-606.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Peptide GAM immunoadsorption in anti-PLA2R positive autoimmune membranous nephropathy. The PRISM Trial. J Clin Apheresis. 2022;37:40-53.
- [CrossRef] [PubMed] [Google Scholar]
- Future landscape for the management of membranous nephropathy. Clin Kidney J. 2023;16:1228-38.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- A randomized study comparing methylprednisolone plus chlorambucil versus methylprednisolone plus cyclophosphamide in idiopathic membranous nephropathy. J Am Soc Nephrol. 1998;9:444-50.
- [CrossRef] [PubMed] [Google Scholar]




