

Translate this page into:
Asymptomatic bacteriuria in Nigerian children with sickle cell anemia
Address for correspondence: Dr. Samuel Ademola Adegoke, Department of Paediatrics and Child Health, Obafemi Awolowo University, Ile-Ife, Osun State, Nigeria. E-mail: adegoke2samade@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Urinary tract infections (UTI) in children with sickle cell anemia (SCA) may result in long term renal dysfunction. The prevalence, potential risk factors, and clinical significance of asymptomatic bacteriuria (ASB) were investigated in 196 Nigerian children with SCA in stable state. These children had clinical evaluation and assessment of their mid-stream urine (MSU) for pyuria, culture, and sensitivity tests; urinalysis for proteinuria, and estimated glomerular filtration rate (eGFR), hematocrit, serum creatinine and uric acid estimation. Children with confirmed ASB were compared with those without ASB. Those with confirmed ASB were monitored for 6 months for persistence of significant growth, development of symptomatic UTI, and evaluation of renal functions. The prevalence of probable and confirmed ASB in this cohort of SCA children were 12.2% and 6.6%, respectively. Confirmed ASB was more prevalent among older (P = 0.046) and female (P = 0.003) SCA children, particularly those with pyuria (odd Ratio, OR = 5.4, 95% confidence interval, CI = 2.7-11.0, P < 0.001) and proteinuria (OR = 1.4, 95% CI = 3.9-8.7, P = 0.006). Previous symptomatic UTI was not associated with ASB. Also, the mean eGFR, serum creatinine, and uric acid were not different in the group with ASB and those without ASB (P > 0.05). At the end of 6 month follow-up, two (15.4%) of the 13 children with ASB had persistence of significant growth, but none develop symptomatic UTI. Also, none of the two with persistent ASB had hypertension or deranged renal function. ASB is a significant problem in older age female SCA children, although renal functions were not different among those with and without ASB. A large scale randomized placebo-controlled trial of conventional treatment for ASB in SCA is advocated to define its long-term clinical significance.
Keywords
Asymptomatic
bacteriuria
children
nigerian
pyuria
sickle cell anaemia

Introduction
Urinary tract infection (UTI) is a major cause of morbidity in children, especially those with sickle cell anemia (SCA), who have impaired immunological state and are susceptible to recurrent infections including UTI.[12] Both symptomatic and asymptomatic UTI in SCA children commonly result from repeated infarctions of the kidney, papillary necrosis, and inability of the kidneys to concentrate urine.[34] This may ultimately lead to chronic kidney disease. In resource poor settings where renal replacement therapy is limited, early detection and management of ASB in SCA children may retard this progression.
Asymptomatic bacteriuria (ASB) is defined as 100,000 or more bacterial colony forming units per milliliter (CFU/ml) of uncentrifuged clean voided mid-stream urine specimen processed within 1 h of collection from a child without symptoms, usually in repeated urine samples.[5] ASB has been found to be more prevalent among children with SCA than their counterparts with normal hemoglobin.[36]
It is important to regularly monitor the pattern of the organisms implicated in childhood UTI, and their antibiotic sensitivity to limit development of chronic kidney disease in this high-risk group of children. However, clinico-laboratory factors facilitating the development of ASB in children with SCA, as well as whether ASB is a warning sign to more serious renal disease in children with SCA are unclear. This present study was undertaken to estimate the prevalence and risk factors to ASB in children with SCA in a University Teaching Hospital. In addition, it sought to determine the immediate clinical significance of ASB in children with SCA.
Materials and Methods
The study population comprised a group of sickle cell anemia children attending the Pediatric hematology clinic of the hospital. In this prospective study, children with SCA in stable state, i.e., free of any crises; were screened for UTI to determine the prevalence, potential determinants, and clinical significance of ASB among them. The study was done over a year period from November 2010 to October 2011. Children who had fever, or any other symptom, whether related or unrelated to urinary tract, or those who had history suggestive of recurrent UTI or use of antibiotics in the previous 2 weeks were not included.
Ethical approval was granted by the Ethics and Research Committee of the hospital, and written consent was obtained from parents and care-givers of each subject.
The socio-demographic characteristics such as age, gender, and social class of the parent were recorded. Also, the frequency of significant painful episode, hospitalization, and transfusion program in the previous 1 year was documented. Significant painful episode, for the purpose of this study was defined as an acute painful event requiring treatment at a healthcare facility or at home with either (a) parenteral or an equianalgesic dose of oral narcotics or (b) parenteral or an equianalgesic dose of oral non-steroidal anti-inflammatory drugs.[7]
Nutritional status was assessed using the National Center for Health Statistics and WHO (NCHS/WHO) definition of wasting, underweight, and stunting.[8] Those with weight-for height below two standard deviations (SD) were categorized as wasted. Blood pressure (BP) was measured with the age-appropriate Accuson mercurial sphygmomanometer by standard techniques. Using the Pediatric Task Force guidelines on BP control, children with systolic and or diastolic BP above the 5th percentile for age, gender, and height were categorized as hypertensive.[9]
Aseptically collected midstream urines (MSUs) were obtained from each patient and sent on the same day within an hour of collection for microbiological analysis. However, urinalysis which was performed on aliquots of the MSU specimen using Combur-9® test strips was done immediately after collection.[10] Proteinuria was defined as a protein reading of trace or greater on dipstick urinalysis.[5] After collection, urine was centrifuged at 2000 revolutions per minute for 5 min, and the sediment was examined for red blood cells, white blood cells, casts, and bacteria.
Bacterial culture was performed by streaking 0.002 mL of the midstream urine with a calibrated loop on MacConkey and 5% sheep blood agar plates.[4] These plates were then incubated at 35°C for 24 h under aerobic conditions.
Isolates were taken as significant if there were ≥105 colony forming unit/mL (CFU/mL) with two or less isolates. Colony counts between 104 and 105 were regarded as doubtful and urine culture was repeated, whereas counts ≤104 CFU/mL were considered as insignificant and therefore taken as negative. Mixed growths of more than two urinary tract pathogens even if in significant quantities, were regarded as contaminated. Identification and antimicrobial susceptibility testing of the significant isolates was done by comparing the zones of inhibition of the test organism.[10]
The patients with significant isolate of at least 105 CFU/mL of a urinary tract pathogen in their first MSU were noted. Second urine samples were collected from these children, i.e., those with significant growth in their first urine sample, and those whose second urine samples yielded significant bacteriuria due to the same urinary tract pathogen with the same sensitivity pattern were regarded as having confirmed asymptomatic bacteriuria. Those whose only the first MSU had significant growth were categorized as having probable ASB.
Renal function was measured with estimated eGFR using Schwartz formula,[11] and determination of serum level of creatinine and uric acid in the laboratory of the hospital by standard procedure.[5] The SCA children with confirmed ASB were assessed at the end of 6 months follow-up for persistence of significant growth in their MSU, development of symptomatic UTI, and evaluation of renal function among those with persistent ASB.
Data analysis
Data were analyzed using Statistical Package for the Social Sciences (SPSS) version 17.0. The prevalence of ASB (the ratio of the number of urines classified as ASB to the total number of collected MSU samples) was determined. Differences in the means of the study variables among those with confirmed ASB and those with sterile urine were determined by independent t-tests and their proportions by Chi-squared tests. Potential predictors of ASB such as age, gender, socioeconomic class, past history of symptomatic urinary tract infection, frequency of significant painful episodes, hospitalization and transfusion in the previous 1 year; nutritional status, steady state hematocrit, proteinuria, and pyuria were determined by logistic regression analysis. Also, differences in the measure of renal functions such as eGFR, serum creatinine, and uric acid of those with and without ASB were determined. The 95 percent confidence interval (95% CI) for this proportion and tests were considered significant if P < 0.05.
Results
Sociodemographic characteristics of children with sickle cell anemia
A total of 196 children with SCA who were eligible for the study were assessed during the period. Their mean age was 7.2 ± 4.0 years, ranging from 2 to 17 years. Ninety-five (48.4%) were younger than 6 years, 54 (27.6%) were aged 6 to 10 years, and 47 (24.0%) were older than 10 years. One-hundred and seven (54.6%) of them were males with a male to female ratio of 1.2:1.
Majority, 165 (84.2%), were from the lower social classes (III-V), and 31 (15.8%) were from the higher social classes (I and II).
Prevalence of asymptomatic bacteriuria
Of the 196 first urine samples examined, 157 (80.1%) had insignificant growth, two (1.0%) had doubtful growth, whereas the remaining 37 (18.9%) had significant growth. All the 37 with significant growths and the two with doubtful growths were cultured again. Of these 39 urine samples, 26 (66.7%) including the initial two with doubtful growths, and 24 of those with initial significant growths had insignificant growth on second culture. Only 13 samples had significant growth on second culture and the patients with those urine were regarded as having confirmed ASB. Twenty-four children whose only first MSU had significant growth were regarded as having probable ASB. Thus, the prevalence of confirmed ASB was 6.6% and that of probable ASB was 12.2%. The probable ASB group was made up of 15 children whose second MSU samples grew organisms that were different from the first urine sample, eight with no further growth, and one with contamination in the second MSU sample.
Isolated organisms and their sensitivity pattern in the children with confirmed asymptomatic bacteriuria
Gram-negative organisms were the commonest organisms isolated from the urine of these patients, with Escherichia coli being the leading organism. It was isolated in seven (53.8%) of the 13 patients with confirmed ASB. Other pathogens isolated were Staphylococcus albus (15.4%), Proteus mirabilis, Streptococcus faecalis, Streptococcus viridians, and Klebsiella pneumoniae (7.7% each). All the organisms were sensitive to Ciprofloxacin and Ofloxacin. Eleven (84.6%) were sensitive to Genticin and Ceftriaxone whereas eight (61.5%) were sensitive to Nitrofurantoin. All were resistant to co-trimoxazole and ampicillin.
Comparison of patients with confirmed asymptomatic bacteriuria and those with sterile urine
Females were 5.5 times more likely to have confirmed ASB compared with males. Eleven (84.6%) of 13 children with confirmed ASB as against 67 (42.1%) of the 159 with sterile urine were females (P = 0.003). Also, higher proportion of older children (school age children and adolescents combined) had confirmed ASB (P < 0.046). However, social class, frequency of significant painful episodes, transfusion, and hospitalization in the previous 1 year, previous symptomatic UTI and severe wasting were not statistically associated with having ASB (P > 0.05). Although more children with confirmed ASB than those with sterile urine had hypertension, the difference was not statistically significant (P = 0.182) [Table 1].
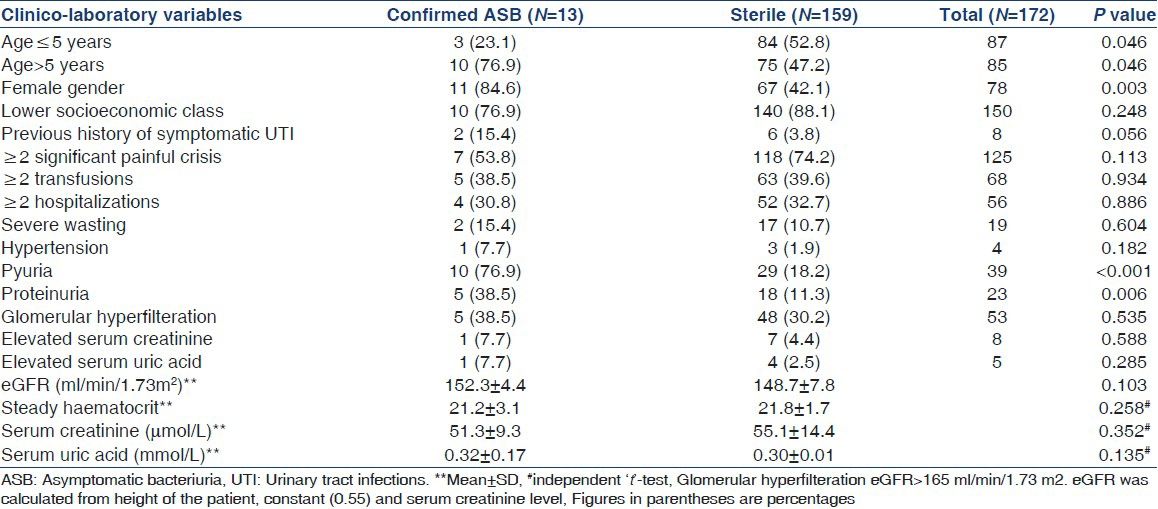
The hematocrit of the group with confirmed ASB and those with sterile urine was similar (21.2 ± 3.1% vs. 21.8 ± 1.7%) respectively; (t = 1.13, P = 0.258). Similarly, there was no statistical difference in the mean eGFR, serum creatinine, and uric acid values between the confirmed ASB group and sterile urine group. However, significantly higher proportion of children with confirmed ASB (38.5% vs. 11.3%, P = 0.006) had proteinuria and pyuria (76.9% vs. 18.2%, P < 0.001) as shown in Table 1.
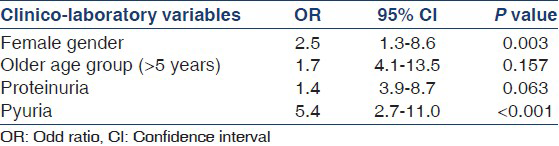
The relationship between the predictors and probability of having ASB was determined by logistic regression analysis. The result shows that female gender (OR = 2.5; 95% CI: 1.3-8.6) and the presence of pyuria (OR = 5.4; 95% CI: 2.7-11.0) best predicted ASB as shown in Table 2.
Follow-up findings
At the end of 6 month of follow-up, while two (15.4%) of the 13 children with confirmed ASB had persistence of significant growth, none developed symptomatic UTI. Also, none of the two with persistent ASB had hypertension or deranged renal function.
Discussion
The prevalence of 6.6% of confirmed ASB in this study is similar to 2.8-6.9% in studies on ASB in SCA, in most parts of the developing countries.[346] The prevalence of probable ASB was however 12.2% in this population of sickle cell patients. The major possible factors associated with the development of ASB in this cohort of children were gender, age, presence of proteinuria, and pyuria.
The gender and age difference in the prevalence of ASB agreed with previous findings both in adults and children.[34] The gender difference has been linked to the relative deficiency of secretory IgA antibody response from the mucosal surface in the urinary tract of females compared with males.[12]
In untreated pregnant women with ASB, about 20-40% of them will eventually develop pyelonephritis, which may lead to prematurity and delivery of low birth weight baby. For non-pregnant females, ASB has a high sensitivity and specificity of predicting a future symptomatic episode of UTI.[13] However, the clinical significance of ASB in children without vesicoureteral reflux, urinary tract obstruction or functional abnormalities of the urinary tract is still debatable.[4613] Among children with normal hemoglobin genotype, ASB is usually considered a benign condition.[1213] Their counterparts who have SCA may indeed develop severe renal damage.[5] This is because SCA patients are already at risk of developing renal cortical scarring, enlarged glomeruli, vascular disorganization of the medulla, and renal functional abnormality such as increased effective renal blood flow and hyperfiltration.[14] These anatomical and physiological abnormalities account for sickle cell nephropathy as well as the high prevalence of chronic kidney disease in sickle cell disease.[14]
In this study, the mean eGFR, serum creatinine, and uric acid were similar among SCA children with ASB and those without ASB. Also, eGFR was not different among the two groups. Although this finding is unexpected, the levels of serum creatinine and uric acid are not usually affected, until glomerular filtration rate decline by about 50%.[15] Also, the small size of the children in the confirmed ASB group may account for the statistical insignificance of these values.
The organisms isolated are similar to the commonly isolated organisms in other studies.[356] In ASB, alterations in the host-pathogen interaction may be responsible for the absence of symptoms, despite the presence of urinary pathogens.[16]
ASB is a significant problem in SCA, especially among older females with proteinuria and pyuria. However, further research particularly; large scale randomized placebo-controlled trials of conventional treatment for ASB in SCA is needed to determine the clinical significance of ASB in SCA children.
Acknowledgment
We thank the Directors and the entire staff of the Microbiology and Chemical Pathology laboratory units of the University Teaching Hospital, Ado-Ekiti for the support and cooperation during the period of the study.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Use of nitrite dipstick test in the screening for urinary tract infection in children. West Afr J Med. 2000;19:206-8.
- [Google Scholar]
- Bacteraemia in homozygous sickle cell disease in Africa: Is pneumococcal prophylaxis justified? Arch Dis Child. 2007;92:21-3.
- [Google Scholar]
- Socio-demographic factors associated with asymptomatic bacteriuria in children with sickle cell anemia in a tertiary health facility in South eastern, Nigeria. Italian J Pediatr. 2011;3:1-5.
- [Google Scholar]
- Asymptomatic bacteriuria in sickle cell disease: A cross-sectional study. BMC Infect Dis. 2006;6:46.
- [Google Scholar]
- Urinary tract infection. In: Azubuike JC, Nkangineme KEO, eds. Paediatrics and Child Health in a Tropical Region (1st ed). Owerri: African Education Service; 1999. p. :326-8.
- [Google Scholar]
- Asymptomatic bacteriuria in children with sickle cell anaemia. Nig J Paediatr. 1988;15:19-25.
- [Google Scholar]
- A brief review of the pathophysiology, associated pain, and psychosocial issues in sickle cell disease. Int J Behav Med. 2005;12:171-9.
- [Google Scholar]
- Malnutrition: Quantifying the health impact at national and local levels. In: WHO Environmental Burden of Disease Series No. 12. Geneva: WHO; 2005. p. :1-51.
- [Google Scholar]
- National high blood pressure education program working group on high blood pressure in children and adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Paediatrics. 2004;114:555-76.
- [Google Scholar]
- Laboratory examination of urine. In: Part 2, District Laboratory Practice in Tropical Countries (2nd ed). London: Cambridge University press; 2000. p. :107-13.
- [Google Scholar]
- New equations to estimate GFR in children with CKD. J Am Soc Nephrol. 2009;20:629-37.
- [Google Scholar]
- Estimation of renal function in diabetic nephropathy.Comparison of five methods. Nephron. 1987;47:36-42.
- [Google Scholar]
- Granulocyte function in women with diabetes and asymptomatic bacteriuria. Diabetes Care. 1997;20:392-5.
- [Google Scholar]




