

Translate this page into:
Awareness level of kidney functions and diseases among adults in a Nigerian population
Address for correspondence: Dr. Okwuonu Chimezie Godswill, Department of Internal Medicine, Nephrology Unit, Federal Medical Center, Umuahia, Abia State, Nigeria. E-mail: getchimezie@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The prevalence of kidney diseases is on the increase in Nigeria. The cost of its management is far beyond the reach of an average patient. Prevention is thus of paramount importance and awareness of kidney diseases will help in its prevention. The aim of this study is to assess the level of awareness of kidney functions and diseases among adults in a Nigerian population. A semi-structured, researcher – administered questionnaire was the tool for data collection. Four hundred and thirty-five questionnaires were analyzed. There were 160 males (36.8%) and 275 females (63.2%). The mean age was 42.8 ± 14 years with a range of 18–78 years. Among these, 82.1% were aware of the kidneys' involvement in waste removal from the body through urine while 36% and 29% were aware of kidneys' role in blood pressure regulation and blood production, respectively. Only 26.6% correctly identified at least two basic functions of the kidneys. Also, 32.6% of the respondents were aware of at least three common causes of kidney diseases in our environment. Majority of the respondents (70.7%) did not know that kidney diseases could be inherited. Furthermore, belief in alternative therapy for kidney disease was documented in 83.2%, while unawareness of dialysis as a treatment modality was recorded in 68% of the respondents. The awareness of kidney functions and diseases among the population is poor. Measures are needed to improve this to stem the rising prevalence of chronic kidney disease in Nigeria.
Keywords
Awareness
dialysis
kidney diseases
kidney functions
Nigeria
transplantation

Introduction
The World Health Organization and Global Burden of Disease (GBD) project report published in 2006 showed that diseases of the kidney and urinary tract contribute to the GBDs – with approximately 850,000 deaths every year and 15,010,167 disability-adjusted life years.[1] The 2010 global ranking of premature causes of death show that kidney diseases moved up from position 32 in 1990 to position 24 in 2010.[2] These findings refer only to the more advanced stages of kidney disease especially end stage renal disease (ESRD). The proportion of patients with milder kidney dysfunction is definitely larger and contributes significantly to cardiovascular mortality.[2]
The cost of management of ESRD is exorbitant and far beyond the reach of an average patient in our community.[3] In Nigeria, as in most other developing countries, there is no social security system or health insurance scheme in place to assist the patient on renal replacement therapy and as such the burden is borne solely by the patient and relatives.[3] Essential treatment such as erythropoietin, active Vitamin D and statins may not be available or affordable.[4] Co-existing conditions such as hepatitis infection, parasitic infestations and malnutrition are common, and transportation difficulties often result in noncompliance to treatment and follow-up visits.[4] Where treatment is frequent as medically required, some patients are faced with the burden of not meeting up with the demands of various employers of labor due to productive hours of work lost to hospital visits.[5] Families are faced with a chronically depressed unemployed relative who must be escorted to a possibly distant dialysis center to receive treatment.[5]
Late presentations to health care facility also contribute to the morbidity and mortality of kidney diseases in Nigeria.[6] Some patients with chronic kidney disease (CKD) initially use herbal medications for treatment and seek help from spiritual houses, only to eventually resort to hospitals and specialists at a stage when the ailment is advanced.[6]
In line with the high morbidity and mortality from CKD and its cost of management, prevention is of paramount importance. The first step toward prevention of any disease is awareness of that disease. Few studies have assessed the awareness level of kidney diseases in Nigerians from the available literature search. Among these include a study carried out by Okaka and Ojogwu among undergraduate nonmedical students in Benin, Nigeria[7] and another by Alebiosu in a representative general population in southwest Nigeria.[8] This is despite the rising prevalence of CKDs recorded in different parts of the country[910111213] with its attendant cost, morbidity and mortality. In this study, we set out to assess the awareness level of kidney diseases among adults in a semi-urban population of Abia state, southeast Nigeria. Our objectives are to assess the knowledge base of the participants as regard to basic functions sub-served by the kidneys, causes of kidney diseases, symptoms of kidney disease as well as knowledge of treatment options of kidney disease.
Materials and Methods
Study design and setting
This is a descriptive cross-sectional questionnaire-based study carried out in Olokoro, a semi-urban community in Umuahia South local government area of Abia state, South East Nigeria. The community is about 8 km from the center of the State capital. The inhabitants are predominantly Igbos, mostly Christians and traders with few civil servants and farmers. The village has nine primary health centers and several patent medicine stores. The houses in the community have primary health care numbers that are used for health-related data acquisition. There are 212 enumeration areas (EA) in Olokoro.
Study population and sample size
The study population included all males and females aged 18 years and above who are resident in the community. Sample size estimation was determined using the formula[14] for estimating minimum sample size for descriptive studies when studying proportions with an entire population size >10,000. An estimated population size of 52,712 individuals was used, based on the recently issued national and state population estimate of Umuahia South.[15] A previous study[7] showed that 25.1% of the participants have good knowledge of kidney diseases. The sample size in this study was extrapolated from this value at a 95% confidence level with a 5% margin of error. This gave a minimum sample estimate of 289 individuals. A sample size of 460 adults was selected to allow for possible nonresponders.
Sampling method
Multi-stage cluster sampling method was carried out using EAs as clusters. Fifteen of these EAs were selected randomly by balloting. Households in the involved EAs were selected by systematic random sampling method. The first household was determined by the spin of a bottle. Thereafter, individuals in each selected household who meet the inclusion criteria were selected for the study.
Study procedure
Structured, researcher – administered questionnaire containing 27 items was the tool for data collection. Twenty-three items on the questionnaire bordered on their knowledge of kidney number, location, basic functions of the kidneys, common symptoms and causes of kidney disease as well as possible treatment modalities. The questionnaire, written in English, was translated to the local dialect by an expert in the local dialect. The translated format was thereafter translated back to English by a second party. The two English versions were then cross-checked for accuracies and consistencies in the questions. The local dialect format was used in the data collection. Face and content validity was evaluated by two Nephrologists and two resident doctors. The interviewers had a common training conducted by the principal investigator to ensure accurate and uniform data collection. A pilot study was conducted among 30 adults in an EA in the community not selected for the study. The aim of the pilot study was to reveal difficulties in understanding the meaning of the questions, estimate the amount of time for completion of the questionnaire and assess the participants' willingness to be involved in the study. Based on the outcome, some questions were adjusted accordingly and “I don't know” was added to some responses. The study lasted 1 month. The study protocol, questionnaires and consent forms were reviewed and approved by the human resource and ethical committee of Federal Medical Center, Umuahia, Abia state, Nigeria.
The outcome variable was awareness level of kidney functions and diseases. This was expressed as overall knowledge score. A score of one was given for each correctly answered question on number, location and functions of the kidney, symptoms of kidney diseases and causes of kidney diseases.
Statistical analysis
The data collected were analyzed using the Statistical Package for Social Sciences version 21.0 (IBM Corp, Armonk, NY, USA). Quantitative variables were expressed as mean ± standard deviation. Qualitative variables expressed as proportions. The number of correct answers out of 23 was used to grade the knowledge level of the respondents as poor knowledge (0–8 correct answers), some knowledge (9–16 correct answers) and good knowledge (17–23 correct answers). Correlation analysis was used to assess for association between knowledge scores, age and educational level. Analysis of variance (ANOVA) was used to assess if mean knowledge scores differed significantly among the occupational groups. P < 0.05 was considered significant.
Results
Four hundred and sixty questionnaires were administered to consenting adults in the community. Up to 449 were turned in giving a response rate of 97%. Among these, 435 were properly filled and used in the analysis.
There were 160 males representing 36.8% of the participants and 275 females, which makes up 63.2% of the participants [Table 1]. The age of the respondents was 42.8 ± 14 years with a range of 18–73 years.

Analysis of the data showed that 90.2% of the respondents knew the correct number of kidneys in the human body. However, only 44% knew the correct location of the kidneys in body. While 43.2% indicated that the kidneys are located in the chest region, 7.6% and 3.2% felt that they are located in the back and head, respectively.
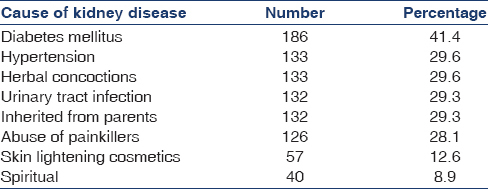
Knowledge of seven possible causes of kidney disease was assessed [Table 2]. Only 32.6% of the respondents were aware of three or more common causes of renal disease. There was a significant but weak positive correlation between educational level of respondents and their knowledge of causes of kidney disease (Spearman's rho = 0.147, P = 0.004). Majority of the respondents (70.7%) did not know that kidney diseases could be inherited.
Also knowledge of three basic functions of the kidneys was sought for and responses were as shown in Figure 1. Only 26.6% of respondents were able to identify at least two of these functions. Only 7.1% of respondents correctly identified all three basic renal functions. There was a significant but weak positive correlation between educational level of respondents and their knowledge of basic renal functions (Spearman's rho = 0.128, P = 0.012).
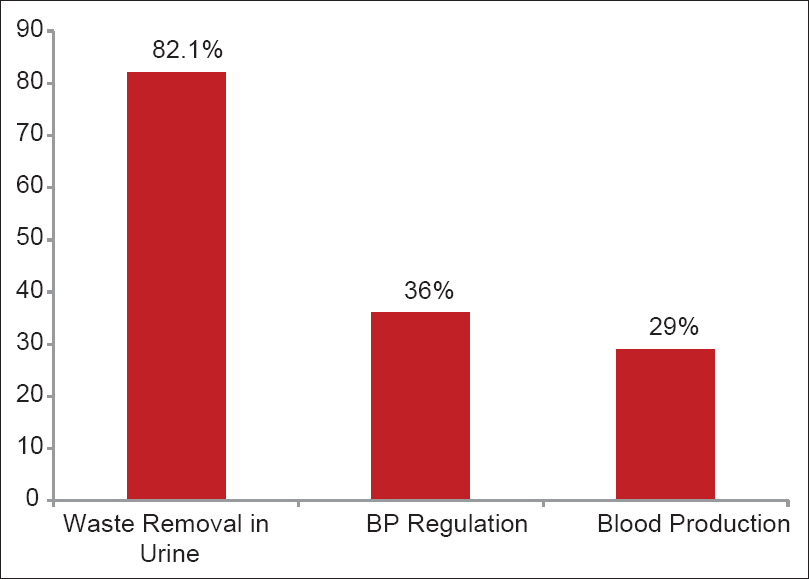
- Respondents' knowledge of functions of the kidneys
Symptoms of kidney disease identified by the participants and their proportions are shown in Figure 2.
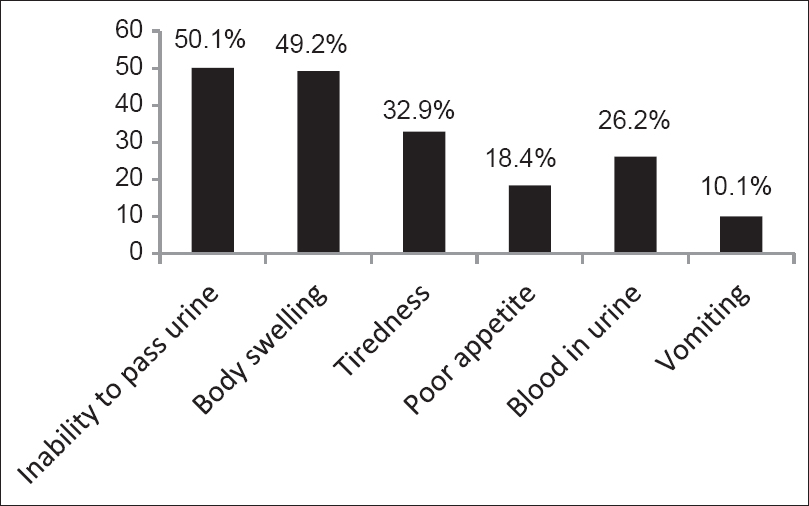
- Respondents' knowledge of symptoms of kidney diseases
Three hundred and sixty-two (83.2%) respondents believe in alternative treatment for kidney disease. However only 171 knew for sure what such treatment entailed. Of this group, 61.4, 26.2, 23.2, 26.5% believed that spiritual, herbal medications, nutritional supplements and water therapy respectively could be used to treat kidney diseases. There was no significant association between educational level and belief in alternative therapy (χ2 with trend = 2.700, P = 0.100).
On treatment options for kidney failure, the awareness of dialysis as a treatment option for kidney disease was generally poor; up to 68% are unaware of it [Figure 3].
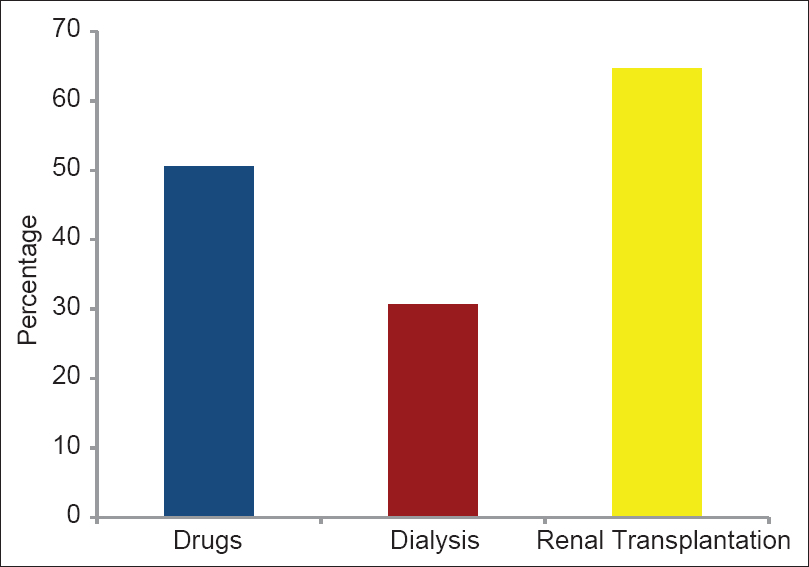
- Knowledge of treatment options for kidney disease
Generally, the awareness level of the respondents of kidney functions and diseases was poor. Analysis showed that more than 60% of the participants in this community had a poor knowledge of kidney functions and disease [Table 3].

There was a significant but weak positive correlation between level of education and overall knowledge score (Spearman rho = 0.156, P = 0.002). There was no correlation between the age of respondents and their overall knowledge (Pearson's coefficient = −0.047, P = 0.325). ANOVA showed there was no difference in overall knowledge among the different occupations (F5429 = 1.091, P = 0.365).
Discussion
In this study, we examined the level of awareness of kidney functions and diseases among a representative adult population in a semi-urban Nigerian population.
The main findings were: (1) The knowledge of the participants on number of kidneys in the human body was good; (2) most respondents (73.4%) demonstrated poor knowledge of basic functions of the kidney; (3) many (67.4%) had poor knowledge of possible causes of kidney diseases; (4) majority of the respondents (76.5%) did not know that kidney disease could be inherited; (5) belief in alternative treatment was recorded in majority of participants (83.2%) having no significant association with their educational level; and (6) more people are aware of kidney transplantation as a treatment option for kidney diseases than dialysis and use of drugs.
This result is similar to that of an earlier study in Southwestern Nigeria among the general populace[8] where 63.8% of the respondents were not aware of the basic functions of the kidneys. This similarity can be accounted for by the comparable sociodemographic characteristics of participants in both studies. However, a similar study done among nonmedical undergraduates at the University of Benin, Nigeria[7] showed a higher level of knowledge of basic functions of the kidney – only 5% of the students had poor knowledge of kidney functions. Most of these students had undertaken biology lessons in secondary schools and have access to health information through books and internet facilities. These are factors that may have accounted for the higher level of knowledge in the study.
The leading causes of kidney disease in Nigeria are hypertension, chronic glomerulonephritis and diabetes mellitus.[16] The participants in this study had poor knowledge of the possible causes of kidney diseases. However, using diabetes mellitus and hypertension as examples and comparing this study with previous studies, there seems to be an improvement in knowledge of the general populace on the causes of kidney diseases over the years.[78] This may be attributed to increased enlightenment from health workers and enlightenment over the media.
The prevalence of hypertension is high globally[17] and in Nigeria.[18192021] It is the second leading cause of ESRD in Nigeria.[1622] Despite this, only 30.6% of the respondents in this study are aware that hypertension can cause kidney disease.
Herbal medications or concoctions have been implicated in some cases of kidney failure in Nigeria.[6] Similarly, painkillers (non steroidal anti inflammatory drugs) have been implicated in some forms of kidney injury just as skin lightening creams is one of the culprits in the etiology of nephrotic syndrome.[23] Our study revealed that only 30.6%, 29% and 13.1% of the respondents associated kidney diseases with herbal concoctions, abuse of painkillers and use of skin lightening creams, respectively. This is alarming, considering the fact that females, the gender mostly associated with use of bleaching creams, constituted more than 60% of our study population. Thus, there is likelihood of increased use of skin lightening creams with this poor awareness. Also, a good number of the participants in our study were farmers and traders. These set of people commonly abuse analgesics due to body aches from the nature of their work. Hence, there is a high possibility of abuse of analgesic and some kidney injury in this population consequent upon their poor knowledge. This poor knowledge level of herbal remedies, skin lightening creams and misuse of painkillers as a cause of kidney disease was also reported by Okaka and Ojogwu.[7] Thus, use of herbal concoctions should be discouraged because most are injurious to the kidneys and their use cannot be monitored. Same should be applied to use of skin lightening creams. In addition, legislation against purchase of unprescribed drugs should be enacted by health policy makers to reduce abuse of painkillers.
Certain forms of kidney diseases such as polycystic kidney disease, medullary cystic disease, Alport syndrome, IgA nephropathy, cystinosis and others can be inherited.[24] It is quite informative that majority of the respondents (70.6%) did not know that kidney diseases could be inherited. This is similar to the findings in the study among undergraduates at the University of Benin, Nigeria, which revealed low level of awareness in up to 94% of the respondents.[7]
In Nigeria, as in some developing countries, patients often present late to heath facilities or not at all for several reasons, which range from prohibitive cost of health care services to use of alternative treatment like spiritual healing and traditional or native healers.[23] Three hundred and sixty-two (83.2%) respondents in this study believe in alternative treatment for kidney disease. Suggested alternatives include nutritional supplements, spiritual healing and water therapy.
Due to the high costs of treatment of kidney disease, most people solicit for financial assistance from philanthropists, religious organizations, mass media and others, so as to undergo kidney transplantation. This may perhaps be the reason why most participants in this study were more aware of kidney transplantation as a treatment option than dialysis.
While sociodemographic factors have been suggested by other studies to influence knowledge of other chronic diseases,[2526] none have explored the relationship between sociodemographic factors and their influence on knowledge of CKD among the general population. This study found that higher educational level was significantly associated with better overall knowledge as well as knowledge in the domains of functions of the kidney and causes of kidney diseases among the participants. This is similar to the finding in a hospital-based study by Chow et al.[27] where overall knowledge levels as well as knowledge in respective domains were associated with education level. The questions used to assess knowledge level are similar for our study and the latter study, and could account for the similarity in result obtained.
Limitation
More than 75% of participants in this study were traders, farmers and students. This group of people do not have a definite weekly or monthly income. Hence, we did not determine the impact of economic status on the awareness level of participants in this study.
Conclusion
This study has revealed a low level of awareness of kidney disease among adults in a semi-urban community of southeast Nigeria. To achieve a meaningful reduction in prevalence of kidney disease in our environment, there is need to increase the knowledge of basic functions of kidneys, common causes of kidney disease, early recognition of symptoms and availability of treatment among our people. This can be achieved through enlightenment campaigns, workshops, seminars, program by religious institutions and mass media. Furthermore, patients must be given a clear understanding of the rationale for every aspect of the therapy in order to keep them participating in any control program. In addition, the government should take definite steps to reduce the cost of drugs and implement health care screening programs at community level for detection of undiagnosed hypertension, diabetes and early stages of kidney diseases.
Source of Support: Nil
Conflict of Interest: None declared.
References
- Global Burden of Disease. Available from: http://www.who.int/whosis/menu.cfm?path
- Investigating the worldwide burden of kidney disease. Available from: http://www.theisn.org
- Cost implications of treatment of end-stage renal disease in Nigeria. J Coll Med. 1998;3:95-6.
- [Google Scholar]
- The enormity of chronic kidney disease in Nigeria: The situation in a teaching hospital in South-East Nigeria. J Trop Med 2010:501957.
- [Google Scholar]
- Traditional herbal preparations and acute renal failure in south west Nigeria. Trop Doct. 1999;29:244-6.
- [Google Scholar]
- Awareness level of kidney diseases among nonmedical students in Benin city, Nigeria. J Med Biomed Res. 2012;11:29-34.
- [Google Scholar]
- The pattern, clinical characteristics and outcome of ESRD in Ile-Ife, Nigeria: Is there a change in trend? Afr Health Sci. 2011;11:594-601.
- [Google Scholar]
- Towards prevention of chronic kidney disease in Nigeria: A community-based study in South East Nigeria. Kidney Int Suppl. 2013;3:195-201.
- [Google Scholar]
- Prevalence of chronic kidney disease and its risk factors among adults in a rural population in Edo state, Nigeria. J US China Med Sci. 2011;8:471-81.
- [Google Scholar]
- Community based screening for chronic kidney disease and its risk factors amongst adults in Howlshe Jos: National Postgraduate Medical College of Nigeria 2009
- Prevalence of chronic kidney disease and its risk factors among adults in a rural population of Kano: West African College of Physicians 2010
- Research Methodology with Statistics for Health and Social Sciences. Ilorin: Nathdex Publication; 2004. p. :115-20.
- Federal Republic of Nigeria. In: Legal Notice on Publication of 2006 Census Final Results, Official Gazette. Vol Vol. 962009. Abuja: National Population Commission; 2010. p. :1-103.
- [Google Scholar]
- Chronic renal failure at the Olabisi Onabanjo University Teaching Hospital, Sagamu, Nigeria. Afr Health Sci. 2006;6:132-8.
- [Google Scholar]
- Global burden of hypertension: Analysis of worldwide data. Lancet. 2005;365:217-23.
- [Google Scholar]
- Undiagnosed hypertension and proteinuria in a market population in Ile-Ife, Nigeria. Arab J Nephrol Transplant. 2011;4:141-6.
- [Google Scholar]
- A prevalence of cardiometabolic risk factors among a rural Yoruba south-western Nigerian population: A population-based survey. Cardiovasc J Afr. 2010;21:26-31.
- [Google Scholar]
- A community-based study of hypertension and cardio-metabolic syndrome in semi-urban and rural communities in Nigeria. BMC Health Serv Res. 2010;10:71.
- [Google Scholar]
- Non Communicable Disease in Nigeria. In: Final Report of National Survey. Lagos: Federal Ministry of Health; 1997. p. :1-118.
- [Google Scholar]
- End-stage renal disease in sub-Saharan and South Africa. Kidney Int Suppl. 2003;63:S119-22.
- [Google Scholar]
- Aetiological relationship between nephrotic syndrome and mercury containing skin lightening creams and medicated soaps. Niger Med J. 2005;46:29-32.
- [Google Scholar]
- Polycystic kidney disease and other inherited tubular disorders. In: Longo DL, Kasper DL, Jameson JL, Fauci AS, Hauser SL, Loscalzo J, eds. Harrison's Principles of Internal Medicine. New York: Mc Graw Hill; 2012. p. :2355-2366. Ch 284
- [Google Scholar]
- Racial differences in hypertension knowledge: Effects of differential item functioning. Ethn Dis. 2009;19:23-7.
- [Google Scholar]
- Diabetes awareness in general population in Cameroon. Diabetes Res Clin Pract. 2010;90:312-8.
- [Google Scholar]
- Limited knowledge of chronic kidney disease among primary care patients - A cross-sectional survey. BMC Nephrol. 2012;13:54.
- [Google Scholar]




