

Translate this page into:
Combined surgical and immunosupressive therapy for encapsulating peritoneal sclerosis
Address for correspondence: Dr. P. K. Bipi, Flat 12 D, Trinity Crown, Trinity 4 C Apartments, Opposite Lulu Mall, Edapally P. O., Ernakulam, Kochi, Kerala, India. E-mail: bipi.pk@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Encapsulating peritoneal sclerosis (EPS) is an infrequent but serious complication of long-term peritoneal dialysis with 50% mortality and lack consensus on treatment. The pathogenesis of EPS is ill understood, and diagnosis lacks specificity and relies on clinical, radiographic and microscopic evaluation. Since there is no general agreement on managing EPS, we report a case treated successfully with surgery followed by immunosuppressive therapy with tamoxifen and steroids. He later successfully underwent deceased donor renal transplantation.
Keywords
Encapsulating peritoneal sclerosis
peritoneal dialysis
treatment

Introduction
Encapsulating peritoneal sclerosis is a rare but potentially fatal complication of continuous ambulatory peritoneal dialysis. The most important risk factor for its development is the duration of peritoneal dialysis. The diagnosis of EPS can be challenging, especially in developing countries due to the high prevalence of tuberculous peritonitis. Once established, PD is usually abandoned. We report a case in which surgery followed by immunosuppressive therapy was effective in treatment.
Case Report
A 14-year-old male, diagnosed as juvenile nephronophthisis was initiated on continuous ambulatory peritoneal dialysis (CAPD) at the age of 7 years. The initial peritoneal equilibration test (PET) test revealed a low transporter status and he had good ultrafiltration. After 3 months of being on CAPD, he underwent a live related renal transplantation at the age of 7 years with the mother as the donor. Unfortunately, he had primary graft failure due to thrombosis of graft renal artery, and he continued CAPD. After about 18 months, he had an episode of fungal peritonitis with candida albicans isolated on culture. CAPD catheter was removed, and he was initiated on hemodialysis via right internal jugular tunneled catheter. After about 5 months, he developed catheter-related blood stream infection not responding to antibiotic therapy requiring removal of hemodialysis catheter, and he was reinitiated on CAPD. Despite four exchanges with 1 L dwell volume, he remained fluid overloaded and the PET test repeated showed high transporter status. Since he had no permanent vascular access, he continued to be on CAPD with fluid restriction and high dose diuretics with occasional hemodialysis support through temporary vascular access. After 54 months of peritoneal dialysis, he started experiencing abdominal symptoms in the form of intermittent abdominal pain, nausea, vomiting, weight loss with abdominal distension. Ultrasound scan of the abdomen revealed moderate ascites with septations. The ascitic fluid study revealed exudative ascites and predominant lymphocytes with negative adenosine deaminase. Antituberculous therapy was started as tuberculosis is highly prevalent and has a similar presentation. CAPD was discontinued, and he was started on hemodialysis. After 2 months of antituberculous therapy, the patient continued to be symptomatic with progressive abdominal pain and abdominal distension. Computed tomography abdomen with oral and intravenous contrast revealed prominent bowel loops with thickened peritoneum [Figure 1] barium meal follow through done revealed dilated small intestine confined mainly to the left side of the abdomen.

- Computed tomography abdomen with oral and intravenous contrast revealed prominent bowel loops with thickened peritoneum
He was taken for explorative laparotomy because of worsening abdominal symptoms. Intraoperatively, there were dense adhesions of bowel loops to the parietal wall and between bowel loops. Omentum was seen plastered onto bowel loops. Adhesions were released and enterolysis done. Peritoneal and omental biopsies wtaken and were sent for histopathological examination. Histopathologic examination revealed adipose tissue cells with large areas of fibrosis, collagenization, inflammatory cells, hemorrhage, and hemosiderin-laden macrophages consistent with sclerosing peritonitis [Figure 2].
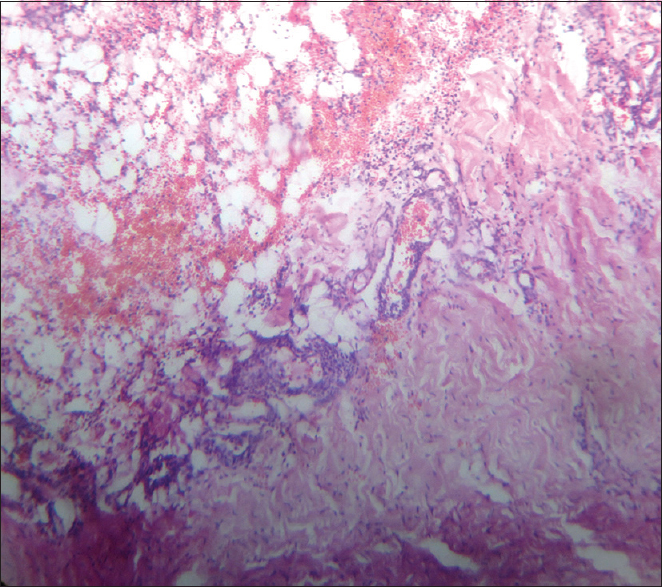
- Histopathologic examination of peritoneal and omental biopsies revealed adipose tissue cells with large areas of fibrosis, collagenization, inflammatory cells, hemorrhage, and hemosiderin laden macrophages consistent with sclerosing peritonitis
Antituberculous therapy was stopped, and oral prednisolone was started at the dose of 1mg/kg/day, tapered gradually after a period of 4 weeks to the maintenance dose of 10 mg/day. He was also started on tamoxifen 10 mg/day. He continued to be on hemodialysis support. During the period, he had abdominal discomfort and was advised small frequent meals. After about 1 year, he received a deceased donor renal allograft with antithymocyte globulin induction and tacrolimus, mycophenolate mofetil and prednisolone for maintenance immunosuppression. Tacrolimus trough levels were maintained at 8–10 ng/mL during the initial 3 months, reduced to 5–8 ng/mL thereafter.
Tamoxifen was continued for another 6 months and stopped. Now almost 16 months since transplantation, he is doing well with normal allograft function (serum creatinine of 0.9 mg/dL) and no abdominal symptoms.
Discussion
Encapsulating peritoneal sclerosis (EPS) characterized by intraperitoneal fibrosis leading to the development of fibrous cocoon that slowly covers the intestine accounting for most of the symptoms. A single most important risk factor is the duration of peritoneal dialysis.[1] Other risk factors identified are higher cumulative glucose exposure,[2] peritonitis,[3] younger age,[4] kidney transplantation,[5] discontinuation of peritoneal dialysis therapy.[6] All these risk factors were present in our patient. The pathophysiology of EPS is best classified as a multiple hit process with vascular endothelial growth factor[7] and transforming growth factor-beta[8] playing a central role. Other factors implicated include fibroblast growth factor (FGF); platelet derived growth factor and tumor necrosis factor. Epithelial-mesenchymal transformation is also thought to play a prominent role in EPS.[9] The clinical presentation almost mimicks the symptomatology of abdominal tuberculosis, and hence, differentiating EPS from abdominal tuberculosis is challenging at least in developing countries where tuberculosis is highly prevalent. Histopathology is vital in differentiation as epithelioid granulomas are demonstrated in the submucosa and serosa in around 90% of cases in tuberculous peritonitis. The typical caseating granulomas are identified in 54.5% cases.[10] Acid fast bacilli in the granuloma were variably reported in as low as 6–8% to as high as 58%. EPS, on the other hand, is characterized by fibrin deposition, fibroblast swelling, extensive fibrosis, capillary neoangiogenesis with perivascular hemorrhage and mononuclear cell infiltration. Immunohistochemical markers of fibroblast proliferation like FGF, macrophage migratory inhibitory factor and bcl 2 were found to be helpful in differentiating EPS from non-EPS cases. However, its usefulness in cases of infectious peritonitis is yet to be established.[11]
The treatment of EPS has evolved over the years. Tamoxifen, a nonsteroidal antioestrogen used in the treatment of fibrosing diseases like retroperitoneal fibrosis has been tried in the treatment of EPS ever since its first successful use in 1992.[12] It is thought to act by stimulating the action of matrix metalloprotease-9 to degrade type 4 and denatured collagen. Since then several case series have been published reporting its successful use in EPS.[1314] Treatment with tamoxifen and steroid was found to improve survival compared to steroid monotherapy alone.[15]
We report this case because of its rarity and the diagnostic challenges it posed to us. The judicious use of clinical symptomatology, supplemented with diagnostic imaging and confirmation by histopathology helped in diagnosing and optimally treating the patient. We also highlight the continuation of surgery and immunosuppressive therapy for a better outcome in the management of EPS in reducing the mortality. The diagnosis of EPS does not preclude future renal transplantation.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Encapsulating peritoneal sclerosis: Incidence, predictors, and outcomes. Kidney Int. 2010;77:904-12.
- [Google Scholar]
- Peritoneal sclerosis in peritoneal dialysis patients related to dialysis settings and peritoneal transport properties. Kidney Int Suppl. 2001;78:S42-7.
- [Google Scholar]
- Risk factors for encapsulating peritoneal sclerosis in patients who have experienced peritoneal dialysis treatment. Clin Exp Nephrol. 2005;9:148-52.
- [Google Scholar]
- Peritoneal sclerosis in chronic peritoneal dialysis patients: Analysis of clinical presentation, risk factors, and peritoneal transport kinetics. Perit Dial Int. 1997;17:136-43.
- [Google Scholar]
- Posttransplant encapsulating peritoneal sclerosis: A worrying new trend? Perit Dial Int. 2007;27:619-24.
- [Google Scholar]
- Encapsulating peritoneal sclerosis in Japan: A prospective, controlled, multicenter study. Am J Kidney Dis. 2004;44:729-37.
- [Google Scholar]
- Vascular endothelial growth factor in peritoneal dialysis: A longitudinal follow-up. J Lab Clin Med. 2001;137:125-32.
- [Google Scholar]
- PAI-1 secretion and matrix deposition in human peritoneal mesothelial cell cultures: Transcriptional regulation by TGF-beta 1. Kidney Int. 1998;54:87-98.
- [Google Scholar]
- Epithelial-to-mesenchymal transition of mesothelial cells is an early event during peritoneal dialysis and is associated with high peritoneal transport. Kidney Int Suppl. 2008;108:S26-33.
- [Google Scholar]
- Abdominal tuberculosis: A histopathological study with special reference to intestinal perforation and mesenteric vasculopathy. J Lab Physicians. 2009;1:56-61.
- [Google Scholar]
- Pathology of encapsulating peritoneal sclerosis. Perit Dial Int. 2005;25(Suppl 4):S19-29.
- [Google Scholar]
- Encapsulating peritoneal sclerosis: Case series from a university center. Korean J Intern Med. 2013;28:587-93.
- [Google Scholar]
- Corticosteroid and tamoxifen therapy in sclerosing encapsulating peritonitis in a patient on continuous ambulatory peritoneal dialysis. Nephrol Dial Transplant. 2004;19:2423-4.
- [Google Scholar]
- The Pan-Thames EPS study: Treatment and outcomes of encapsulating peritoneal sclerosis. Nephrol Dial Transplant. 2009;24:3209-15.
- [Google Scholar]




