

Translate this page into:
Concurrent renal tuberculosis and renal cell carcinoma: A coincidental finding
Address for correspondence: Dr. M. G. Manoj, Department of Pathology, Armed Forces Medical College, Pune, Maharashtra, India. E-mail: manoj.gopal@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
The association of tuberculosis and renal adenocarcinoma is uncommon.[1] While the incidental discovery of renal cell carcinoma (RCC) in a tuberculous kidney is well-described, the discovery of tuberculous lesions after nephrectomy for cancer is exceptional.[1] We describe a case in which histological examination revealed associated tuberculosis.
A 32-year-old male was investigated for incidental renal mass. He underwent a partial nephrectomy on 17 June 2008. The specimen was nodular and measured 6.0 cm × 4.0 cm × 2.0 cm. The cut-surface showed a nodule with multiple tiny cysts and central yellowish areas. The tumor was encapsulated having solid and tubular patterns. Tumor cells were round to polygonal, having abundant clear to focally granular cytoplasm and deserving a Fuhrman grade 1 [Figure 1a]. On immunohistochemistry, tumor cells were positive for pancytokeratin (AE1/AE3) [Figure 1b] and vimentin, and negative for cytokeratin 7 and CD 10. Among the tumor lobules were several epithelioid cell granulomas surrounded by lymphocytes. Occasional granulomas showed central caseation necrosis and few Langerhan’s type of giant cells. Ziehl Neelson (ZN) stain for acid fast bacilli and stains for fungal organisms were negative. However, PCR for tuberculosis on the tissue was positive. The individual was further investigated and administered anti-tubercular therapy for 6 months. He is on a regular follow-up and is doing well.
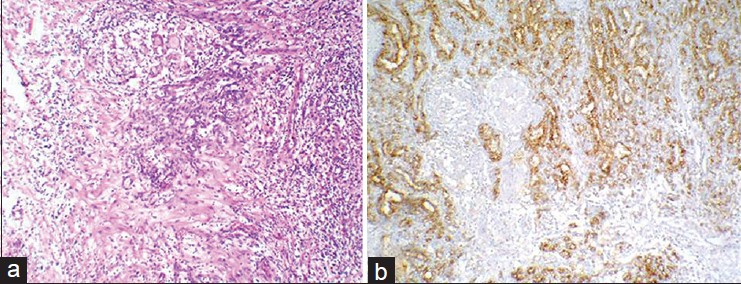
- Epithelioid cell Granulomas were dispersed within conventional RCC (Fuhrman grade 1) with an intense chronic inflammation (H and E, × 100); (b) Cytokeratin positive RCC cells with dispersed epithelioid cell granulomas (Immunohistochemistry for AE1/AE3 panCK positive renal carcinoma cells, ×100)
Granulomas with unknown etiology and without secondary changes like necrosis are designated as sarcoid-like forms. The distinction between a tumor-related granulomatous reaction and true sarcoidosis can be a problematic issue.[2] Such lesions have been described in association with lymphoma and other solid tumors.[3] Khurram et al,[4] studied a series of breast carcinomas with associated granulomatous reaction in lymph nodes with or without necrosis. In all cases, ZN stain for AFB and PAS stain for fungus were negative. Six of the 12 cases that had granulomas with necrosis were positive for Mycobacterium tuberculosis (MTB)-DNA, while 5 of 10 cases without necrosis were also positive for MTB-DNA. This correlates well with our findings of presence of a RCC with granulomas showing presence of MTB-DNA. Al-Assiri et al., found RCC and squamous cell carcinoma to coexist in a tuberculous kidney.[5]
Very few cases of RCC in tuberculous kidneys have been reported. An ultrasonography of the abdomen and pelvis is recommended in cases of renal tuberculosis as an adjunct to early diagnosis of RCC.
References
- Renal tuberculosis and renal adenocarcinoma: A misleading association. Prog Urol. 2002;12:89-91.
- [Google Scholar]
- Renal cell carcinoma with sarcomatoid features and peritumoral sarcoid-like granulomatous reaction: Report of a case and review of the literature. Int J Surg Pathol. 2008;16:345-8.
- [Google Scholar]
- Conventional renal cell carcinoma with granulomatous reaction: A report of three cases. Virchows Arch. 2003;443:220-1.
- [Google Scholar]
- Breast cancer with associated granulomatous axillary lymphadenitis: A diagnostic and clinical dilemma in regions with high prevalence of tuberculosis. Pathol Res Pract. 2007;203:699-704.
- [Google Scholar]
- Renal pelvis squamous cell carcinoma and renal cell carcinoma in a tuberculous kidney. Scientific World Journal. 2004;4:965-8.
- [Google Scholar]




