

Translate this page into:
Incidentally Detected Primary Squamous Cell Carcinoma of Kidney Arising from Renal Pelvis Impersonating Xanthogranulomatous Pyelonephritis
Corresponding author: Archana Shetty, Department of Pathology, Dr. Chandramma Dayananda Sagar Institute of Medical Education and Research (CDSIMER), Dayananda Sagar University, Ramanagara, Karnataka, India. Email: archanashetty2924@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Shetty A, Gunadal S, Edupuganti HS, Harshan TR. Incidentally Detected Primary Squamous Cell Carcinoma of Kidney Arising from Renal Pelvis Impersonating Xanthogranulomatous Pyelonephritis. Indian J Nephrol. 2024;34:410-1. doi: 10.25259/ijn_11_24
Dear Editor,
A 55-year-old male presented with a palpable non-tender mass in the left loin region. Urine examination showed pus cells with culture being positive for Escherichia coli. Ultrasound, contrast-enhanced computed tomography (CECT), and Diethylenetriaminepentaacetate (DTPA) renogram suggested a non-functioning kidney possibly due to xanthogranulomatous pyelonephritis (XGP). Simple nephrectomy was performed. [Figure 1a and b]. Microscopy showed moderately differentiated infiltrating squamous cell carcinoma arising from pelvis (PT4Nx) extending into renal capsule, peripelvic fat, and Gerota’s fascia. Ureteric lining showed complete squamous metaplasia [Figure 1c and d]. At present, six months postoperatively patient is undergoing cisplatin-based chemotherapy and is asymptomatic.
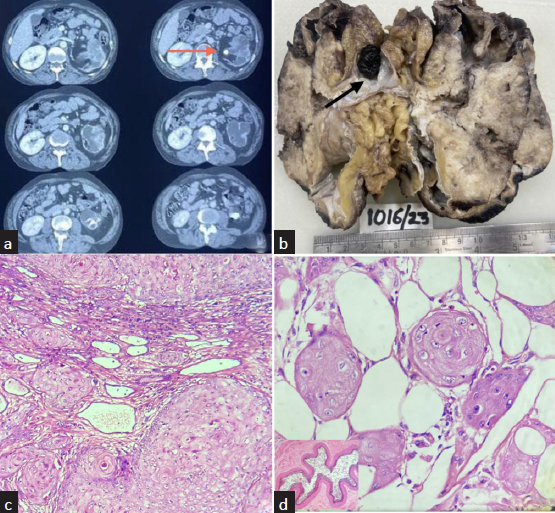
- (a) Serial slice of computed tomogrpahy showing left kidney (orange arrow) showing a hydronephrotic kidney with cortical thinning and stone at pelvi-ureteric junction. (b) Cut section of nephrectomy specimen showing loss of corticomedullary differentiation with dilated calyces and an impacted stone (black arrow) at pelviuretric junction. (c) Microphotograph showing moderately differentiated squamous cell carcinoma invading atrophic tubules (H&E ×40). (d) Squamous cell carcinoma infiltrating the perinephric fat. (H&E 40×) Inset-Ureter with lumen displaying complete squamous metaplasia of the lining epithelium. (H&E ×10).
Squamous cell carcinoma (SCC) of the renal pelvis is associated with chronic irritation to the epithelial lining of urothelium secondary to stones, infection, and inflammation leading to squamous metaplasia, dysplasia, and eventually SCC.1,2 Akin to clinical features, radiological findings in SCC are non-specific.3 As it is impractical to perform CT for every patient with renal stone, intravenous urography (IVU) should be carried out periodically, especially in patients with long-standing stones. Filling defects, delay in appearance of pyelogram or renal parenchymal thickening in IVU may indicate a renal tumor despite the absence of mass effect warranting further investigations.2
Microscopically, primary renal SCC resembles SCCs at other sites.4 The conspicuous presence of adjacent flattened urothelial keratinized squamous metaplasia in association with dysplasia supports the diagnosis of primary SCC of the renal pelvis.5 Regardless of parenchymal or pelvic origin, surgical resection is regarded as the mainstay of treatment. The prognosis of renal SCC is generally poor.6
In our case, primary renal SCCs were underdiagnosed as XGP with pelviureteric junction calculus as CECT showed contracted thickened renal pelvis with dilated calyces mimicking bear’s paw sign - classically as described for XGP. Furthermore, XGP is commonly seen in cases of chronic obstruction, which was also present in our case. As the diagnosis of SCC then becomes incidental during histopathological examination, a high index of suspicion for this rare malignancy in cases with long-standing obstructive stones with non-characteristic areas of enhancement on contrast is recommended by the clinicians. Radical nephrectomy and lymph node dissection may be the only option to treat suspected SCC, which may also help eliminate additional procedures.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
References
- Incidentally detected squamous cell carcinoma of renal pelvis in patients with staghorn calculi: Case series with review of the literature. ISRN Oncol. 2011;2011:620574.
- [CrossRef] [PubMed] [Google Scholar]
- Renal calculus complicated with squamous cell carcinoma of renal pelvis: Report of two cases. Can Urol Assoc J. 2015;9:E310-2.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Primary squamous cell carcinoma of the kidney: A case report and review of the literature. Afr J Urol. 2020;26:79.
- [Google Scholar]
- Primary squamous cell carcinoma of the kidney parenchyma with ascending colon invasion: A case report and literature review. Int J Surg Case Rep. 2022;91:106762.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Primary squamous cell carcinoma of the kidney: A case report and review of the literature. Afr J Urol. 2020;26:79.
- [Google Scholar]
- Prmary squamous cell carcinoma of the kidney parenchyma with ascending colon invasion: A case report and literature review. Int J Surg Case Rep. 2022;91:106762.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




