

Translate this page into:
Delayed Malposition of a Split-Tip Tunneled Cuffed Hemodialysis Catheter
Corresponding author: Zaheer Amin Virani, Institute of Renal Sciences, Gleneagles Global Hospital, Mumbai, Maharashtra, India. E-mail: zarockin@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Virani ZA, Vishnoi S, Vadlapatla K, Yeleshwaram VR. Delayed Malposition of a Split-Tip Tunneled Cuffed Hemodialysis Catheter. Indian J Nephrol. doi: 10.25259/IJN_52_2024.
A 66-year-old male with diabetes, hypertension, and chronic kidney disease was initiated on hemodialysis (HD) via a right internal jugular vein (IJV) tunneled cuffed hemodialysis catheter (TCHC) in 2018. In August 2021, he presented with suboptimal blood flows during his prior two dialysis sessions and with partial extrusion of the TCHC. The TCHC cuff, as well as some part of the stem, was out.
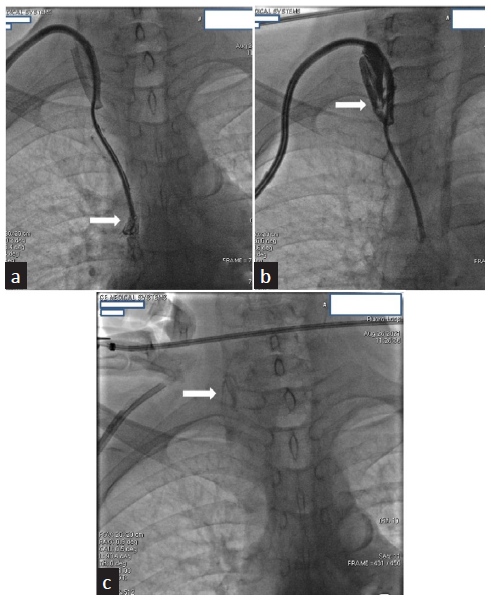
A chest X-ray revealed malposition of the catheter, with one tip going down in the superior vena cava [SVC] and the other going up probably in the right IJV [Figure 1a]. A previous chest CT scan done 3 months ago for pneumonia was reviewed. It showed a normally placed right-sided TCHC with both its tips in right atria [Figure 1b].
![(a) Shows a chest x-ray with a malpositioned catheter, with one tip in the superior vena cava [SVC] and the other tip in the right IJV (white arrows). (b) Shows a CT reconstructed lateral image of the chest with a normally placed right-sided TCHC with both its tips in right atria (white arrow). (c) Shows a malpositionedTCHC with one tip in the right IJV and the other tip in SVC (white arrows). (d) White arrow shows a TCHC with one tip folded onto itself (white arrow).](/content/170/2024/0/1/img/IJN_52_2024-g1.png)
- (a) Shows a chest x-ray with a malpositioned catheter, with one tip in the superior vena cava [SVC] and the other tip in the right IJV (white arrows). (b) Shows a CT reconstructed lateral image of the chest with a normally placed right-sided TCHC with both its tips in right atria (white arrow). (c) Shows a malpositionedTCHC with one tip in the right IJV and the other tip in SVC (white arrows). (d) White arrow shows a TCHC with one tip folded onto itself (white arrow).
Fluoroscopy revealed one tip had folded onto itself, retrograde to the blood flow, going into the right IJV and the other tip was in SVC [Figure 1c and 1d]. Dye injected through the venous port was seen exiting freely from the tip in SVC without any filling defect [Figure 2a]. Dye injected via the arterial port exited from the misplaced tip in right IJV with filling defects [Figure 2b].
- (a) Shows dye injected through the venous port of the TCHC exits from the tip in SVC without any filling defect (white arrow). (b) Shows dye injected via the arterial port exits from the misplaced tip in right IJV with filling defects (white arrow). (c) White arrow shows a remnant thrombus in the right IJV.
This TCC was gently pulled out under fluoroscopic vision without much resistance. Despite continuous negative pressure aspiration during TCC removal, a remnant of thrombus was seen left behind in the right IJV [Figure 2c]. A new 23-cm right IJV TCHC was inserted. The procedure was uneventful, and good flows were documented in both lumens. Dialysis was performed without any complications and the patient was discharged on the same day.
Delayed mechanical complications of TCC insertion are fibrin sheath formation, catheter occlusion, catheter impingement or fragmentation, damage to the port chamber, and malposition.1 Symmetrical tip and step-tip catheters have a lesser risk of malposition than split tip catheters.1
It has been stipulated that the arterial lumen is more prone to malposition during insertion due to lack of guidewire guidance.2 In our case, there is a delayed malposition, which leads to the possibility of occlusion of the arterial lumen by a thrombus, leading to the malposition.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
References
- Complications of central venous port systems: A pictorial review. Insights Imaging. 2019;10:86.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Epidemiology of haemodialysis catheter complications: A survey of 865 dialysis patients from 14 haemodialysis centres in henan province in China. BMJ Open. 2015;5:e007136.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




