

Translate this page into:
Granulomatous Interstitial Nephritis – A Series of Six Cases
Address for correspondence: Dr. Moumita Sengupta, 244 AJC Bose Road, Kolkata - 700 020, West Bengal, India. E-mail: moumitasengupta83@gmail.com
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Granulomatous interstitial nephritis is an uncommon variant accounting for about 6% of all tubulointerstitial nephritis. The etiology can be drugs such as antibiotics and nonsteroidal anti-inflammatory drugs and infections such as tuberculosis, sarcoidosis, and fungal infections. Renal biopsy remains the gold standard for establishing the diagnosis. Here, we present a series of six cases of granulomatous interstitial nephritis, of which two cases were associated with lupus nephritis and another two cases with crescentic glomerulonephritis. Focal segmental glomerulosclerosis and mesangiosclerosis with chronic tubulointerstitial nephritis were detected in the rest of the cases. Most of the patients presented with features of nephrotic syndrome. Urine analysis showed albuminuria in all cases. In renal biopsy, interstitial epithelioid cell granuloma was a constant feature along with which there were foci of necrosis and moderate fibrosis in few cases. But none of our cases had any relevant history of prolonged drug intake. Tuberculosis and fungal infections were also ruled out. Thereby in this case series, we subgroup all the cases into two category four cases associated with granulomatous nephritis and two cases with idiopathic granulomatous nephritis.
Keywords
Granulomatous interstitial nephritis
idiopathic
native kidney biopsy

Background
Tubulointerstitial nephritis can occur due to varied reasons, with granulomatous interstitial nephritis (GIN) being one of the type. Due to its rarity, various literatures reported this entity. Among the known causes of GIN, drug toxicity plays a crucial role, for example, sulfonamides, vancomycin, ciprofloxacin, and fluoroquinolones. Other reported causes are tuberculosis (TB), sarcoidosis, granulomatous vasculitis, gout, and so on. Here, we present six cases of GIN with varied clinical scenario.
Case Series
A total of six cases of GIN were diagnosed over 6 months. Among which four cases were female and two cases were male. Their ages ranged from 14 to 65 years. Out of these six cases, two had lupus nephritis and two pauci-immune crescentic glomerulonephritis. The remaining two cases showed focal segmental glomerulosclerosis (FSGS) and mesangiosclerosis with chronic tubulointerstitial nephritis. The clinicopathological features of the cases are summarized in Table 1.
| Category | SL no. | Age/ Sex | Clinical features | Histopathological findings | Immunofluorescence findings | Other investigations | Diagnosis |
|---|---|---|---|---|---|---|---|
| Idiopathic granulomatous nephritis (n=2) | 1. | 19 years/male | Generalized body swelling Oliguria Hematuria |
Mixed inflammatory cell infiltration and occasional epithelioid cell granuloma with foci of necrosis noted in the interstitium | Only IgM shows segmental positivity in the mesangium | S. Cr - 1.2 S. albumin - 2.0 BUN - 38 Urinary albumin - (++) TB was ruled out by TB PCR |
FSGS with granulomatous interstitial nephritis |
| 2. | 21 years/female | Facial puffiness B/L pedal edema Oliguria |
Marked fibrosis with epithelioid cell granuloma noted in interstitium | Negative | S. Cr - 2.19 S. albumin - 1.8 S. cholesterol - 300 Urinary albumin - (++) TB was ruled out by TB PCR |
Mesangiosclerosis with granulomatous tubulointerstitial nephritis | |
| Cases associated with granulomatous interstitial nephritis (n=4) | 1 | 14 years/female | Facial puffiness Bipedal swelling Rapid rise in serum creatinine |
Ill-defined collection of epithelioid cells and mixed inflammatory cells noted; foci of necrosis identified | IgA, IgG, and C3c show (1+) positivity along mesangium and peripheral capillary wall | S. Cr - 7.13 S. albumin - 2.4 BUN - 60 Urinary albumin - (+++) Urinary RBC - (+++) TB was ruled out by TB PCR |
Pauci-immune crescentic glomerulonephritis with granulomatous interstitial nephritis |
| 2. | 34 years/female | Adult onset nephrotic syndrome | Interstitium shows fibrosis with focal epithelioid cell granuloma and mixed inflammatory cell infiltration | Full-house positivity | S. Cr - 0.9 Urinary albumin - (+++) Urinary RBC – 20-25 ANA - (+++) TB was ruled out by TB PCR |
Lupus nephritis class IV (s), A/C | |
| 3. | 25 years/male | Anasarca Proteinuria Known case of SLE |
Marked fibrosis and noncaseating epithelioid granuloma seen in the interstitium | IgG, C1q, and C3c show granular positivity along GBM | S. Cr - 1.85 S. albumin - 2.2 BUN - 78 ANA - (+++) ANCA - (−ve) C3-61.3 Urinary albumin - (+++) TB was ruled out by TB PCR |
Lupus nephritis class III (A/C) | |
| 4. | 65 years/female | Fever Cough Hemoptysis Anasarca Oliguria Sepsis Diabetic Hypertensive |
Marked fibrosis and chronic inflammatory cell infiltration along with epithelioid cell granuloma formation seen in the interstitium | IgG and C3c show positivity along mesangium and GBM | S. Cr - 3.02 S. albumin - 1.9 ANA - (−ve) MPO ANCA - (++++) PR3 ANCA - (−ve) Urinary albumin - (++) TB was ruled out by TB PCR |
Pauci-immune crescentic glomerulonephritis |
FSGS: Focal segmental glomerulosclerosis; BUN: Blood urea nitrogen; TB: Tuberculosis; PCR: Polymerase chain reaction; RBC: Red blood cell; SLE: Systemic lupus erythematosus
Most of the patients presented with features of adult onset nephrotic syndrome. Two of which showed active sediment as well. One of them was a known case of systemic lupus erythematosus, who presented with classical extrarenal features. One patient had some associated features such as fever, cough, and signs of infection. No history of a specific drug intake over a prolonged period was found. Serum creatinine, urinary albumin, antinuclear antibody (ANA), MPO antineutrophilic antibody (ANCA), PR3 ANCA, and complement proteins were monitored in each case. Serum creatinine was found to be high in most of the cases (66%), among which two cases showed rapidly progressive renal failure. Urinary albumin was raised in each case. Urinary red blood cell was found to be positive in two cases. ANA level was found to be high in two cases, whereas we also got a case with MPO ANCA positivity. In each case, we excluded TB by polymerase chain reaction (PCR) method, and fungal infection was ruled out by periodic acid schiff (PAS) stains.
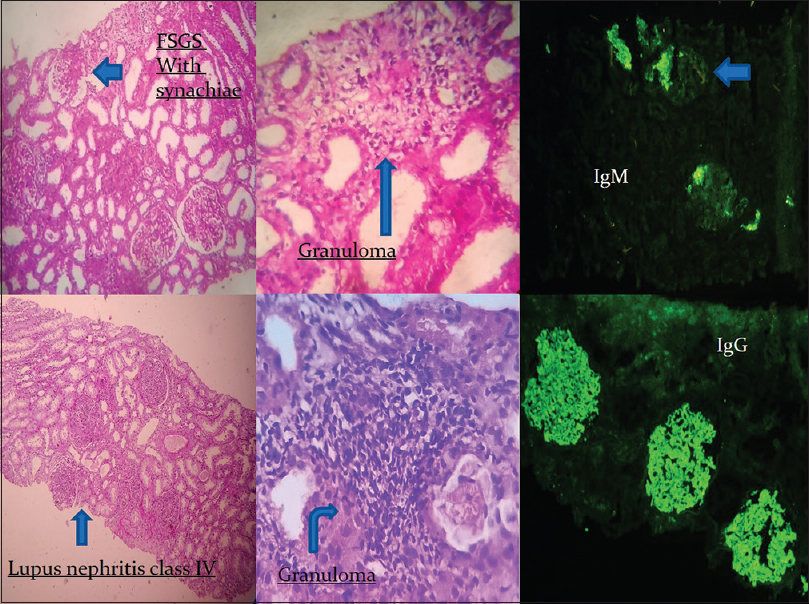
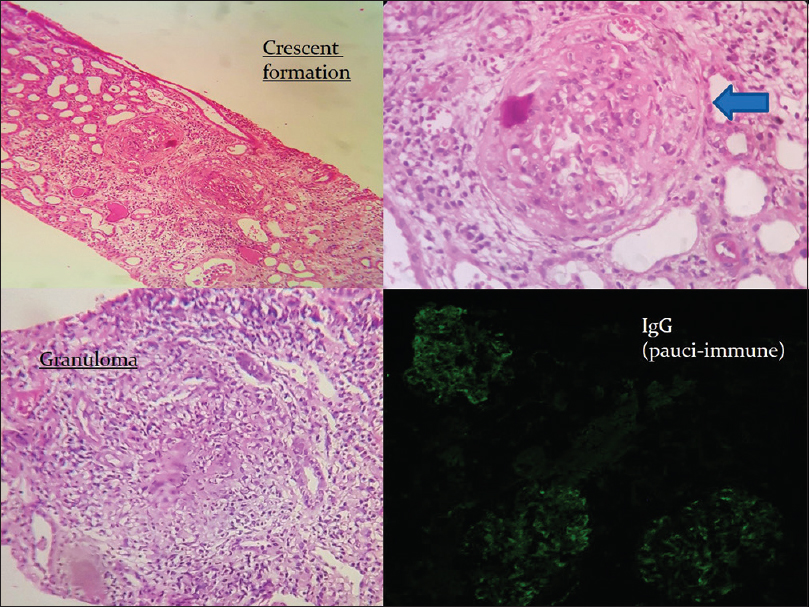
Patient with lupus nephritis revealed mesangial and endocapillary proliferation with irregular membrane thickening in addition to the granuloma formation in the interstitium Figure 1. Immunofluorescence showed full-house positivity with all the antibodies. In the other two cases, we got mesangial matrix expansion and sclerosis in the glomeruli along with the granuloma in the interstitium. In the third and sixth cases, we found crescents in more than 50% of the glomeruli, but no satisfactory immune deposits were noted. Thereby these cases were labeled as pauci-immune crescentic glomerulonephritis Figure 2. In each case, epithelioid cell granuloma formation with marked mononuclear inflammatory cell infiltration in the interstitium was observed. Foci of necrosis were noted in two cases. Moderate interstitial fibrosis and tubular atrophy were detected in two cases which corroborated with raised serum creatinine level.
- Two cases of idiopathic granulomatous interstitial nephritis
- Case of pauci-immune crescentic glomerulonephritis
Discussion
Granulomatous interstitial nephritis is a rare type accounting for about 6% of all tubulointerstitial nephritis.[1] GIN accounts for 0.3%–<1% of all renal biopsies performed.[23] Here, we describe our experience of six cases of GIN over a 6-month period from a tertiary care center in Eastern India.
The etiologies include TB, sarcoidosis, and drugs. Antibiotics and nonsteroidal anti-inflammatory drugs are the usual causes for drug-induced GIN.[4] Some of the antibiotics reported to cause GIN are gentamycin, vancomycin, cefuroxime, clarithromycin, nitrofurantoin, and ciprofloxacin.[5] However, very often no cause could be detected. These cases therefore can be regarded as idiopathic GIN. In our study, we did not get any specific drug history or any specific cause in two cases. The rest of the four cases were associated with either lupus nephritis or pauci-immune crescentic glomerulonephritis.
India being endemic for TB, there are reports suggesting TB as the most common etiology.[67] In a similar report, Colvin et al. showed that among 34 cases of GIN, the most common cause was drug allergy followed by sarcoidosis, and in nine cases no cause could be identified.[2] In spite of clinical history, appropriate investigations, and histology, an etiology could not be defined in some cases which were labeled as “idiopathic GIN.” Idiopathic GIN accounts for 8%–50% of all GIN in various studies. In our study, we found all our cases to be idiopathic.[1238]
GIN is a less common cause of renal allograft dysfunction. Ozdemir et al. reported tubulointerstitial nephritis in 8% of patients presented with graft dysfunction, three of which had GIN.[9] The etiologies of GIN in the renal allograft are infections (mycobacteria and fungi) due to immunocompromised state and antibiotics.[10] We have not reported any graft biopsy.
Conclusion
Determination of the etiology of granulomatous interstitial nephritis is very much crucial for initiation of appropriate therapy. Although TB is the most common cause of granulomatous nephritis in India, chances of getting a granuloma are very rare on renal biopsies. Multiplex PCR for TB DNA in renal tissue is supportive for the diagnosis. Clinical suspicion, radiology, and necrotizing granuloma help us in distinguishing TB from sarcoidosis. Hence, we should keep our threshold of suspicion low to reach a diagnosis in time and start appropriate therapy to preserve renal function.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Granulomatous interstitial nephritis and Crohn's disease. Clin Kidney J. 2016;9:556-9.
- [Google Scholar]
- Clarithromycin-induced granulomatoustubulo-interstitial nephritis. Nephrol Dial Transplant. 2006;21:2654-5.
- [Google Scholar]
- Granulomatous interstitial nephritis: Our experience of 14 patients. Indian J Nephrol. 2013;23:415-8.
- [Google Scholar]
- Renal failure due to granulomatous interstitial nephritis in native and allograft renal biopsies: Experience from a tertiary care hospital, Renal Failure. 2014;36(9):1468-70.
- Granulomatous interstitialnephritis: A clinicopathologic study of 46 cases from a single institution. Int J Surg Pathol. 2006;14:57-63.
- [Google Scholar]
- Renal allograft granulomas in the early post-transplant period. NDT Plus. 2010;3:397-401.
- [Google Scholar]
- Granulomatous tubulointerstitial nephritis in therenal allograft. Am J Kidney Dis. 2000;36:E27.
- [Google Scholar]




